INTRODUCTION
What is the ACE medical system?
The Advanced Combat Environment 3 Medical system overhauls and converts Arma 3's medical features and systems to a much more realistic, immersive and challenging experience. The ACE3 Medical system features two mission-dependant medical system settings: basic or advanced. The settings of each can be tweaked. We however use the advanced medical features in the pursuit of making medical gameplay more engaging, and enjoyable, especially for our combat lifesavers, which becomes more prominent.
Why Advanced?
It is a system designed to add complexity, challenge, and value to medical elements of Arma 3, as we decided that the basic system is not suited to our gameplay style due to its excessive speed and over-simplicity.
An additional incentive to not get shot is added through adding treatments which only medical classes can provide. Advanced medical introduces the following on top of what the basic system adds as a foundation:
• Basic simulation of medications
• Blood loss depending on injury severity and size
• Vital signs
• More accurate player hitpoint values
• Tourniquet
• Heart rate & blood pressure
• More than 4 treatment methods as opposed to basic
In ACE the human body is represented as 6 distinct areas that can receive damage. Some of these areas have special abilities such as applying a tourniquet or using a variety of IV solutions.
Each living person in the battlespace has four key metrics which define their state of health. Every action you take will be to maintain or restore one of these metrics:
• Blood Volume
• Pulse
• Oxygen saturation
• Responsive State (Are they conscious?)
Besides the 4 elements introduced by basic medical, advanced (w/KAT) introduces the following:
• More detailed wound system.
• Accurate blood loss based upon sustained injuries.
• Vitals, including heart rate and blood pressure.
• Cardiac Arrest.
• Airway Management
• Breathing
• Circulation
• Various treatment methods such as CPR, different kinds of IVs and a working tourniquet.
An additional incentive to not get shot is added through adding treatments which only medical classes can provide. Advanced medical introduces the following on top of what the basic system adds as a foundation:
• Basic simulation of medications
• Blood loss depending on injury severity and size
• Vital signs
• More accurate player hitpoint values
• Tourniquet
• Heart rate & blood pressure
• More than 4 treatment methods as opposed to basic
In ACE the human body is represented as 6 distinct areas that can receive damage. Some of these areas have special abilities such as applying a tourniquet or using a variety of IV solutions.
Each living person in the battlespace has four key metrics which define their state of health. Every action you take will be to maintain or restore one of these metrics:
• Blood Volume
• Pulse
• Oxygen saturation
• Responsive State (Are they conscious?)
Besides the 4 elements introduced by basic medical, advanced (w/KAT) introduces the following:
• More detailed wound system.
• Accurate blood loss based upon sustained injuries.
• Vitals, including heart rate and blood pressure.
• Cardiac Arrest.
• Airway Management
• Breathing
• Circulation
• Various treatment methods such as CPR, different kinds of IVs and a working tourniquet.
EQUIPMENT, MYTHS, AND DEFINITIONS
Recommended Table of Equipment
Note that this is only a recommendation and should be treated as such. Understand that personal preference and mission type should be considered when selecting equipment for the mission.
15 — 40 × Field Dressing
15 — 40 × Elastic Bandage
15 — 40 × Packing Bandage
15 — 40 × QuikClot
15 — 40 × Sterile Gauze Bandage
10 × Morphine Autoinjector
10 × Epinephrine Autoinjector
10 × Tourniquet (CAT)
4 × Saline IV (250ml)
3 × Saline IV (500ml)
2 × Saline IV (1000ml)
1 × Surgical Kit
1 × AED X-Series or Pulse Oximeter
1 × Accuvac
10 × AAT Kit
10 × King LT
10 × Chest Seal
10 × Splint
10 × Naloxone
10 × Amiodarone
10 × Lidocaine
10 × Atropine
10 × Ammonium Carbonate
10 × Tranexamic Acid
10 × Ondansetron
2 - 12 × 16g IV
2 × 20g IV
2 - 4 × 45mm IO / Fast IO
1 - 5 × Personal Aid Kit (Check the medical settings for this)
1 × Mag light equivalent
2-3 × White smokes
1-2 × Blue/Green smokes
15 — 40 × Elastic Bandage
15 — 40 × Packing Bandage
15 — 40 × QuikClot
15 — 40 × Sterile Gauze Bandage
10 × Morphine Autoinjector
10 × Epinephrine Autoinjector
10 × Tourniquet (CAT)
4 × Saline IV (250ml)
3 × Saline IV (500ml)
2 × Saline IV (1000ml)
1 × Surgical Kit
1 × AED X-Series or Pulse Oximeter
1 × Accuvac
10 × AAT Kit
10 × King LT
10 × Chest Seal
10 × Splint
10 × Naloxone
10 × Amiodarone
10 × Lidocaine
10 × Atropine
10 × Ammonium Carbonate
10 × Tranexamic Acid
10 × Ondansetron
2 - 12 × 16g IV
2 × 20g IV
2 - 4 × 45mm IO / Fast IO
1 - 5 × Personal Aid Kit (Check the medical settings for this)
1 × Mag light equivalent
2-3 × White smokes
1-2 × Blue/Green smokes
Common Myths
• CPR does not wake up unconscious people - never true: It only brings them out of cardiac arrest. If the patient has a heart rate, CPR isn't going to help.
• Helmets are effective - previously false: Now helmets can make the difference between life and death. However, a helmet will not stop a bullet that hits you directly in the face.
• Splints do not affect PAK time - previously true: Previously it could help, now it does not help. Fractures are caused by damage, but don't count as damage, therefore not contributing to the PAK time.
• Blood loss does not affect stamina usage.
• Running doesn’t increase bandage falloff chance.
• High heart rate and High blood pressure doesn't affect one's ability to wake up.
• Helmets are effective - previously false: Now helmets can make the difference between life and death. However, a helmet will not stop a bullet that hits you directly in the face.
• Splints do not affect PAK time - previously true: Previously it could help, now it does not help. Fractures are caused by damage, but don't count as damage, therefore not contributing to the PAK time.
• Blood loss does not affect stamina usage.
• Running doesn’t increase bandage falloff chance.
• High heart rate and High blood pressure doesn't affect one's ability to wake up.
Definitions
• "Pull Security”: Keeping your gun up, and looking outward away from triage. Constantly scanning the area for anything that may pose a threat to friendly forces.
• “Stable”: If the person can be left alone and not die, he is stable. Specifically, he is not bleeding and his medication will not kill him. (Consciousness is only secondary)
• “Unstable”: If the person can't be left alone due to uncontrolled bleeding or medication.
• “Category”: Category of patient’s injuries:
CAT1: The patient is combat effective (small bruises, scrapes, pain, controlled bleeding).
CAT2: The patient is combat ineffective (bleeding controlled or minimum, broken limbs, severe weapon sway, unconscious + stable).
CAT3: The patient is at an immediate risk of death (heavy bleeding, cardiac arrest, unconscious + unknown medical status)
CAT4: The patient is dead. KIA.
• “Stable”: If the person can be left alone and not die, he is stable. Specifically, he is not bleeding and his medication will not kill him. (Consciousness is only secondary)
• “Unstable”: If the person can't be left alone due to uncontrolled bleeding or medication.
• “Category”: Category of patient’s injuries:
CAT1: The patient is combat effective (small bruises, scrapes, pain, controlled bleeding).
CAT2: The patient is combat ineffective (bleeding controlled or minimum, broken limbs, severe weapon sway, unconscious + stable).
CAT3: The patient is at an immediate risk of death (heavy bleeding, cardiac arrest, unconscious + unknown medical status)
CAT4: The patient is dead. KIA.
MEDIC TACTICAL SOP
Medic Outside of Triage
There is typically only one medic per squad, your safety directly affects the ability of your group. If you die their job becomes infinitely more difficult, maybe even impossible. Therefore as a medic YOUR health is more important than anyone else's. The following is how you can keep yourself safe in a mission:
IF YOUR SQUAD IS STATIONARY the best way to keep yourself safe is to keep away from the front lines, finding a suitable triage is also extremely important and as buildings tick both of these boxes they should be your first choice. However buildings will not always be available, in this situation try and find natural cover, a large rock or ditch will suffice in a pinch. In all cases remember to mark your triage position on the map, and to clearly announce it over the radio. It is worth noting that although a medic should under no circumstance seek out the enemy, if engaged you SHOULD seek to protect yourself, your triage, and the people within.
IF YOUR SQUAD IS MOVING staying in one place is not an option, the ways in which a squad can move vary, and your actions will have to adapt depending on the situation.
IF YOUR SQUAD IS MOVING BY VEHICLE get into the central vehicle (or rear vehicle if only 2 are available), and ask any injured troops to get in with you, you can treat them on route. Once you have arrived at your destination set up in the nearest safe location and complete the triage process, (please note that the nearest safe place may be the vehicle.) It is worth remembering that people might not hear your call asking about medical, so it is important to check people's medical menus when in transit.
IF YOUR SQUAD IS MOVING ON FOOT your behavior will have to change depending on the situation, these situations can be boiled down to two unique environments. The first being when you are traveling on foot from one objective to another, and the second being when your squad is town clearing.
WHEN TRAVELING, try and stay as close to the middle of the squad as you can, as it is by far the safest spot available. If possible also try and stay close to your SL when moving a triage point isn't exactly convenient and the next best thing is their "actual marker". If someone is injured you can rendezvous there, or at least use it as a point of reference, once you have met up with the injured party you can then treat them accordingly.
WHEN TOWN CLEARING your actions will have to vary. If the town is a small one a triage is feasible, however due to the risk of severe injury going up drastically when in CQB, be prepared to venture out of your triage at all times.
In medium to large sized towns a triage is out of the question. In this situation it is best to stick with your SL, people with injuries can come straight to you, or if that isn't possible you can ask for their position in regards to the "actual marker" and (if it is safe to do so) head to them. This advice only works if your SL does not engage in CQB, if they do, then you cannot follow. In this situation, your best strategy is to move from cleared building to cleared building, preferably keeping a one building gap between you and the rest of the squad. If someone is injured they can simply hold position until it is clear for you to advance.
Additional Notes
• As a general rule medics DO NOT DRIVE . (A few exceptions would be if you are PLT medic, or if you are driving a short distance through a cleared town ton pick up the squad, however the latter is at your discretion.)
• The medic should always take the safest seat available in a vehicle, this is normally a seat inside the vehicle towards the back. It should NOT be a GUNNER SEAT or a COMMANDER SEAT.
• In any environment if your squad is splitting up for a prolonged period of time, it is advised that you go with the group who is likely to need you the most. Remember to take your own safety into consideration when making this decision, and once you have decided remember to alert your SL.
• It is also incredibly important that you choose carefully, as moving from one group to another later on may prove to be extremely dangerous.
IF YOUR SQUAD IS STATIONARY the best way to keep yourself safe is to keep away from the front lines, finding a suitable triage is also extremely important and as buildings tick both of these boxes they should be your first choice. However buildings will not always be available, in this situation try and find natural cover, a large rock or ditch will suffice in a pinch. In all cases remember to mark your triage position on the map, and to clearly announce it over the radio. It is worth noting that although a medic should under no circumstance seek out the enemy, if engaged you SHOULD seek to protect yourself, your triage, and the people within.
IF YOUR SQUAD IS MOVING staying in one place is not an option, the ways in which a squad can move vary, and your actions will have to adapt depending on the situation.
IF YOUR SQUAD IS MOVING BY VEHICLE get into the central vehicle (or rear vehicle if only 2 are available), and ask any injured troops to get in with you, you can treat them on route. Once you have arrived at your destination set up in the nearest safe location and complete the triage process, (please note that the nearest safe place may be the vehicle.) It is worth remembering that people might not hear your call asking about medical, so it is important to check people's medical menus when in transit.
IF YOUR SQUAD IS MOVING ON FOOT your behavior will have to change depending on the situation, these situations can be boiled down to two unique environments. The first being when you are traveling on foot from one objective to another, and the second being when your squad is town clearing.
WHEN TRAVELING, try and stay as close to the middle of the squad as you can, as it is by far the safest spot available. If possible also try and stay close to your SL when moving a triage point isn't exactly convenient and the next best thing is their "actual marker". If someone is injured you can rendezvous there, or at least use it as a point of reference, once you have met up with the injured party you can then treat them accordingly.
WHEN TOWN CLEARING your actions will have to vary. If the town is a small one a triage is feasible, however due to the risk of severe injury going up drastically when in CQB, be prepared to venture out of your triage at all times.
In medium to large sized towns a triage is out of the question. In this situation it is best to stick with your SL, people with injuries can come straight to you, or if that isn't possible you can ask for their position in regards to the "actual marker" and (if it is safe to do so) head to them. This advice only works if your SL does not engage in CQB, if they do, then you cannot follow. In this situation, your best strategy is to move from cleared building to cleared building, preferably keeping a one building gap between you and the rest of the squad. If someone is injured they can simply hold position until it is clear for you to advance.
Additional Notes
• As a general rule medics DO NOT DRIVE . (A few exceptions would be if you are PLT medic, or if you are driving a short distance through a cleared town ton pick up the squad, however the latter is at your discretion.)
• The medic should always take the safest seat available in a vehicle, this is normally a seat inside the vehicle towards the back. It should NOT be a GUNNER SEAT or a COMMANDER SEAT.
• In any environment if your squad is splitting up for a prolonged period of time, it is advised that you go with the group who is likely to need you the most. Remember to take your own safety into consideration when making this decision, and once you have decided remember to alert your SL.
• It is also incredibly important that you choose carefully, as moving from one group to another later on may prove to be extremely dangerous.
Triage Process
Triage - sorting who needs you first (order of precedence)
• Any unstable patients (including yourself; unstable means here the patient is bleeding)
• Patients in cardiac arrest
• Unconscious patients
• Conscious but closed wounds (needing a stitch)
• Conscious but broken limbs (needing a splint)
• Final treatments (PAK)
• Any unstable patients (including yourself; unstable means here the patient is bleeding)
• Patients in cardiac arrest
• Unconscious patients
• Conscious but closed wounds (needing a stitch)
• Conscious but broken limbs (needing a splint)
• Final treatments (PAK)
STEP 1: IS THE PATIENT RESPONSIVE?
Yes: Ask him if he has wounds / he is in pain. | No: Go to step 2.
STEP 2: IS THE PATIENT BLEEDING?
Yes: Treat the wounds and go to step 3. | No: Skip this step.
STEP 3: IS THE PATIENT BREATHING?
Yes: Go to step 4. | No: Clear the airway
STEP 4: IS THE BLOOD OXYGEN SATURATION GOOD?
Yes: Go to step 5. | No: check for a Pneumothorax and treat if needed
STEP 5: DOES THE PATIENT HAVE A PULSE?
Yes: Go to step 6. | No: Perform CPR, or use an AED (do not touch the Patient when using the AED)
STEP 6: DID THE PATIENT LOSE A LOT OF BLOOD?
Yes: Give fluids. | No: Go to step 7.
STEP 7: IS THE PATIENT IN PAIN?
Yes and stable pulse: Give him morphine. | No: Go to step 8.
Yes and unstable heart rate: Stabilize the heart rate before administering morphine.
STEP 8: IS THE PATIENT AWAKE NOW?
Yes: You’re done. | No: Go to Step 1.
Yes: Ask him if he has wounds / he is in pain. | No: Go to step 2.
STEP 2: IS THE PATIENT BLEEDING?
Yes: Treat the wounds and go to step 3. | No: Skip this step.
STEP 3: IS THE PATIENT BREATHING?
Yes: Go to step 4. | No: Clear the airway
STEP 4: IS THE BLOOD OXYGEN SATURATION GOOD?
Yes: Go to step 5. | No: check for a Pneumothorax and treat if needed
STEP 5: DOES THE PATIENT HAVE A PULSE?
Yes: Go to step 6. | No: Perform CPR, or use an AED (do not touch the Patient when using the AED)
STEP 6: DID THE PATIENT LOSE A LOT OF BLOOD?
Yes: Give fluids. | No: Go to step 7.
STEP 7: IS THE PATIENT IN PAIN?
Yes and stable pulse: Give him morphine. | No: Go to step 8.
Yes and unstable heart rate: Stabilize the heart rate before administering morphine.
STEP 8: IS THE PATIENT AWAKE NOW?
Yes: You’re done. | No: Go to Step 1.
TRIAGE
Triage will be performed at all levels. Traditional categories of triage are immediate, delayed, minimal, and expectant. To easily remember the order of the categories, use the acronym IDME. No significant treatment should occur in the triage area. Casualties should be rapidly sent to the appropriate treatment area for care.
TIMERS
• Revive Timer: 600 seconds
• Breathing timer: 300 seconds
Triage will be performed at all levels. Traditional categories of triage are immediate, delayed, minimal, and expectant. To easily remember the order of the categories, use the acronym IDME. No significant treatment should occur in the triage area. Casualties should be rapidly sent to the appropriate treatment area for care.
TIMERS
• Revive Timer: 600 seconds
• Breathing timer: 300 seconds
Triage in the Field

If you have to treat someone in an unsafe location, check their medical menu immediately. You must now decide if they can reach a safe location in their current condition.
IF THEY CAN, splint their leg if required, pop smoke and head for the nearest suitable triage location.
IF THEY CAN'T, get them to the nearest cover and stabilize them, once you are satisfied with their condition, move them to the nearest suitable triage location.
IF THEY CAN, splint their leg if required, pop smoke and head for the nearest suitable triage location.
IF THEY CAN'T, get them to the nearest cover and stabilize them, once you are satisfied with their condition, move them to the nearest suitable triage location.
Interfacing & Treating
n order to start treating another player, hold down your ACE interaction key (Windows key by default) while looking at the player in question. Healing particular body parts can be done by looking at the part you need to treat, eg, left leg. If you see no option to treat the patient’s left leg, you are likely out of range and will need to move yourself or the patient closer. Patient note: stay still when you're being treated. To the left of your screen, you will see a brief overview of your patient. This will also appear in self-interaction. You will a list of injuries and applied equipment/treatments (in this case a tourniquet). Below it is a log of actions you have performed on the patient.
The icon for a wounded body part will appear red or yellow. Red icons indicate the body part is seriously wounded. Yellow icons indicate the body part is lightly wounded. You will be granted a list of treatments available to you as you hold your ACE interaction key whilst looking at a wounded body part. These treatments will depend on your role and what supplies you have. Some treatments, eg IV, may be available only to combat lifesaver classes.
By default, you can access the ACE medical menu by pressing H. It will give a detailed self-diagnostic as to your status. Looking at another player and pressing H will provide the same interface but it will show the vitals of the player you were looking at.
The icon for a wounded body part will appear red or yellow. Red icons indicate the body part is seriously wounded. Yellow icons indicate the body part is lightly wounded. You will be granted a list of treatments available to you as you hold your ACE interaction key whilst looking at a wounded body part. These treatments will depend on your role and what supplies you have. Some treatments, eg IV, may be available only to combat lifesaver classes.
By default, you can access the ACE medical menu by pressing H. It will give a detailed self-diagnostic as to your status. Looking at another player and pressing H will provide the same interface but it will show the vitals of the player you were looking at.
Priority
In general, the treatment priority is as follows (from most-urgent to least-urgent).
IMMEDIATE
• Bleeding and unconscious. These players may bleed to death if not treated. The player administering the treatment may even often call for help in bandaging the patient, to make sure that the bleeding stops before the patient bleeds out.
• Life-threatening Bleeding. A conscious but bleeding players could pass out or die if not treated. Therefore, anyone bleeding severely is a high priority for treatment.
• Not breathing. A player has 300 seconds before death if not breathing,
DELAYED
• Unconscious but not bleeding. Unconsciousness is somewhat dangerous in and of itself and needs to be treated with some haste. Death from unconsciousness, however, is rarer. Furthermore, once the unconscious player is revived, he may be able to provide cover for the medic during the rest of the treatment.
• Severe Pain. A player in severe pain may pass out, requiring more treatment. Therefore, it may be necessary to administer Morphine to them before that can happen.
MINIMAL
• Minor Bleeding. Minor bleeding can worsen over time and even lead to unconsciousness and death, but it is not immediately life-threatening. Soldiers with minor bleeding may even be able to treat themselves.
• Crippled Legs. Players with crippled legs have a bare minimum of mobility. Leaving them in this state could cause them to fall behind if the unit needs to leave the area, and should be treated sooner rather than later.
• Crippled Arms. Players with crippled arms are not very combat effective. Treatment of this injury will restore one player - and his gun - back to effectiveness.
• Mild Pain. Mild pain in itself is not life-threatening and reduces a player's effectiveness only mildly. Furthermore, Morphine is in short supply, and medics may choose not to treat Mild Pain at all in order to conserve it for more serious cases.
EXPECTANT
• Multiple bleeding wounds, not breathing, cardiac arrest
If there are more than one wounded, treating the Expectant may cause the death of other wounded, a decision to not treat may be necessary.
• Bleeding and unconscious. These players may bleed to death if not treated. The player administering the treatment may even often call for help in bandaging the patient, to make sure that the bleeding stops before the patient bleeds out.
• Life-threatening Bleeding. A conscious but bleeding players could pass out or die if not treated. Therefore, anyone bleeding severely is a high priority for treatment.
• Not breathing. A player has 300 seconds before death if not breathing,
DELAYED
• Unconscious but not bleeding. Unconsciousness is somewhat dangerous in and of itself and needs to be treated with some haste. Death from unconsciousness, however, is rarer. Furthermore, once the unconscious player is revived, he may be able to provide cover for the medic during the rest of the treatment.
• Severe Pain. A player in severe pain may pass out, requiring more treatment. Therefore, it may be necessary to administer Morphine to them before that can happen.
MINIMAL
• Minor Bleeding. Minor bleeding can worsen over time and even lead to unconsciousness and death, but it is not immediately life-threatening. Soldiers with minor bleeding may even be able to treat themselves.
• Crippled Legs. Players with crippled legs have a bare minimum of mobility. Leaving them in this state could cause them to fall behind if the unit needs to leave the area, and should be treated sooner rather than later.
• Crippled Arms. Players with crippled arms are not very combat effective. Treatment of this injury will restore one player - and his gun - back to effectiveness.
• Mild Pain. Mild pain in itself is not life-threatening and reduces a player's effectiveness only mildly. Furthermore, Morphine is in short supply, and medics may choose not to treat Mild Pain at all in order to conserve it for more serious cases.
EXPECTANT
• Multiple bleeding wounds, not breathing, cardiac arrest
If there are more than one wounded, treating the Expectant may cause the death of other wounded, a decision to not treat may be necessary.
Communication
Communicating is very helpful in any situation. You should talk to your patients, whenever you are treating them or gathering information on their medical status while treating another.
Talking about what you are doing can help the patients, and others around you, gives them the ability to know their own status. Don't be scared to do the same to someone unconscious, having someone talking to them can help chase off some boredom of being unconscious.
Just let the players around you know who you are treating and what you are doing.
Examples: "Name, bandaging right leg.", "Name, giving 500 blood.", "Name, PAKing.", "Name, PAK, 50%.",
"Name, You're good/green."
You can refrain from saying the name of the patient if you only have one patient to take care of and that they are aware of it, just make sure to say the patient's name when you start having more patients.
Talking about what you are doing can help the patients, and others around you, gives them the ability to know their own status. Don't be scared to do the same to someone unconscious, having someone talking to them can help chase off some boredom of being unconscious.
Just let the players around you know who you are treating and what you are doing.
Examples: "Name, bandaging right leg.", "Name, giving 500 blood.", "Name, PAKing.", "Name, PAK, 50%.",
"Name, You're good/green."
You can refrain from saying the name of the patient if you only have one patient to take care of and that they are aware of it, just make sure to say the patient's name when you start having more patients.
BASIC TRAUMA CARE ITEMS
Understanding of Different Bandages
Bandage Effectiveness
Refer to the following chart. The four available bandages have varying effectiveness depending on the wound type and size (The higher the effectiveness the better).
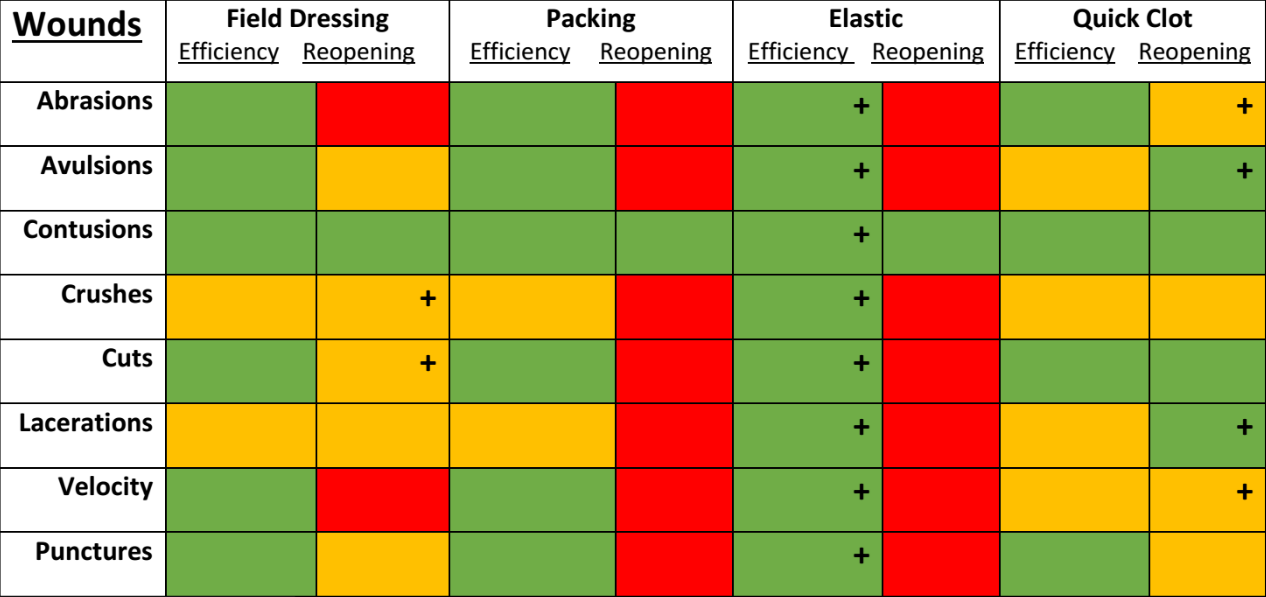
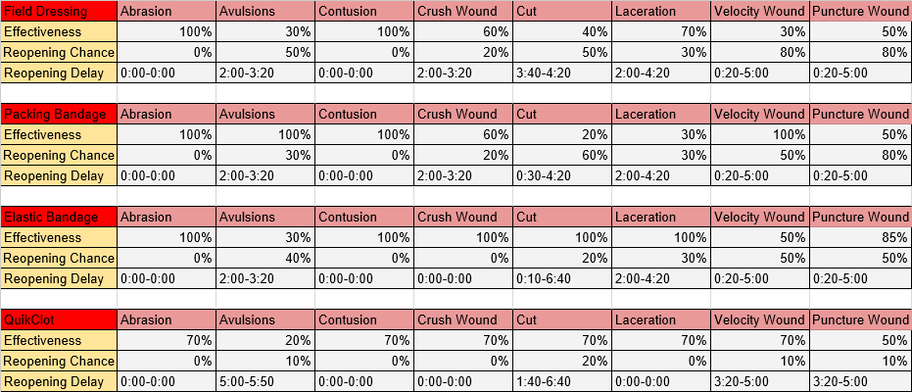
Most combat related wounds are velocity, avulsions and puncture wounds. These are best treated with elastic bandages and quick clot.
Below is a reference of basic information on the understanding of each bandage.
Below is a reference of basic information on the understanding of each bandage.
Field Dressing

A field dressing or battle dressing is a bandage intended to be carried by servicemembers for immediate use in case of (typically gunshot) wounds. It consists of a large pad of absorbent cloth, attached to the middle of a strip of thin fabric used to bind the pad in place. Field dressings are generally issued in sealed waterproof pouches to keep them clean and dry; the pouch can be torn open when required.
Some combat medical technicians make use of field dressing wrappers in the management of "sucking" chest wounds. In such wounds, the working of the chest sucks air through the wound into the space around the lung, rather than sucking air down the throat and into the lung. The hole must be sealed to enable the casualty to breathe properly. As a battlefield interim measure, the waterproof wrapper of a field dressing can be placed over the hole, with the clean inside against the wound, and taped in place. Tape is applied to the sides and top of the wrapper, leaving the bottom edge free. The wrapper then acts as a simple flapper valve, preventing air being sucked in but allowing any that has already entered to be forced out as the casualty exhales.
Some combat medical technicians make use of field dressing wrappers in the management of "sucking" chest wounds. In such wounds, the working of the chest sucks air through the wound into the space around the lung, rather than sucking air down the throat and into the lung. The hole must be sealed to enable the casualty to breathe properly. As a battlefield interim measure, the waterproof wrapper of a field dressing can be placed over the hole, with the clean inside against the wound, and taped in place. Tape is applied to the sides and top of the wrapper, leaving the bottom edge free. The wrapper then acts as a simple flapper valve, preventing air being sucked in but allowing any that has already entered to be forced out as the casualty exhales.
Packing Bandage

Packing bandages, otherwise known as alginate dressings, are made to offer effective protection for wounds that have high amounts of drainage, and burns, venous ulcers, packing wounds, and higher state pressure ulcers. These dressings absorb excess liquid and create a gel that helps to heal the wound or burn more quickly. Containing sodium and seaweed fibres, these dressings are able to absorb high amounts of fluid, plus they are biodegradable after use.
In real life, these dressings require changing around every two days, sometimes more, due to the amount of liquid that they absorb and the nature of the wound. Changing them too often could cause too much dryness or could lead to bacteria penetrating the wound. These should only be used for wet wounds with high liquid drainage; else they can hinder healing by drying out wounds too quickly.
In real life, these dressings require changing around every two days, sometimes more, due to the amount of liquid that they absorb and the nature of the wound. Changing them too often could cause too much dryness or could lead to bacteria penetrating the wound. These should only be used for wet wounds with high liquid drainage; else they can hinder healing by drying out wounds too quickly.
Elastic Bandages

Elastic bandages (also known as compression bandages) are designed to put gentle, even pressure on the tissue around an injury to decrease pain and swelling. It also gives support to an injured area. It is generally used for the compression part of RICE—rest, ice, compression and elevation—the gold standard of first aid treatment for bruises and sprains. Probably the most common brand name for an elastic bandage is an "ace wrap". Elastic bandages help in compressing a new injury or inflammation and help keep swelling down.
Elastic bandages come in many different sizes and lengths. They may come with metal clips or tape to fasten it in place.
Elastic bandages come in many different sizes and lengths. They may come with metal clips or tape to fasten it in place.
QuikClot

QuikClot is a hemostatic agent wound dressing that contains an agent that promotes blood clotting. QuikClot hemostatic devices are different from standard surgical gauzes and other hemostatic agents. They stop bleeding significantly faster and are more effective than standard gauzes and they are just as safe and intuitive to use. They are the most commonly used agent for gunshot & stab wounds.
QuikClot was originally available as a granulate to be poured directly on a wound to stem bleeding. It absorbed the water in the blood, thus increasing its already present clotting capabilities, while also activating platelets. Later it was formulated using zeolite beads, which promoted clotting directly through activation of the coagulation cascade. QuikClot devices are impregnated with kaolin, an inorganic mineral that accelerates the body's natural clotting ability, and produces no exothermic reaction. The product consists of a non-woven gauze coated in kaolin which can be applied to the region of trauma to promote clotting without an exothermic reaction.
QuikClot was originally available as a granulate to be poured directly on a wound to stem bleeding. It absorbed the water in the blood, thus increasing its already present clotting capabilities, while also activating platelets. Later it was formulated using zeolite beads, which promoted clotting directly through activation of the coagulation cascade. QuikClot devices are impregnated with kaolin, an inorganic mineral that accelerates the body's natural clotting ability, and produces no exothermic reaction. The product consists of a non-woven gauze coated in kaolin which can be applied to the region of trauma to promote clotting without an exothermic reaction.
Sterile Gauze

Gauze Bandages are used to help keep a wound clean while still allowing air to ventilate the bandage and skin and help the wound to heal. The woven fabric nature of the bandage is what makes it effective in ventilating. It also makes it absorbent which is useful as it helps prevent excess moisture around the wound site.
Gauze bandages come in many sizes and types. They can be used on wounds where infection is already present and in the process of treatment. They can be combined with topical medicines for such purposes. There are many variations of gauze types for different purposes. Some are multi-layered while others are more simple.
The second factor is gauze roll sterility: non-sterile and sterile. Sterile gauze rolls are provided in their own special individual packaging that is airtight. Non-sterile gauze will be either packaged loose in paper wrapping and plastic cups, or loosely packed in sleeves. Non-sterile gauze is typically used for secondary wrap -- an absorber that backs a primary dressing to take up any exudate should it soak through the first layer. It can also be used as a primary dressing with an antiseptic topping. Sterile gauze is to be used in direct contact with the wound and will have the lowest chance of cross-contamination as it is hermetically sealed, making it preferable for burn wounds.
Gauze bandages come in many sizes and types. They can be used on wounds where infection is already present and in the process of treatment. They can be combined with topical medicines for such purposes. There are many variations of gauze types for different purposes. Some are multi-layered while others are more simple.
The second factor is gauze roll sterility: non-sterile and sterile. Sterile gauze rolls are provided in their own special individual packaging that is airtight. Non-sterile gauze will be either packaged loose in paper wrapping and plastic cups, or loosely packed in sleeves. Non-sterile gauze is typically used for secondary wrap -- an absorber that backs a primary dressing to take up any exudate should it soak through the first layer. It can also be used as a primary dressing with an antiseptic topping. Sterile gauze is to be used in direct contact with the wound and will have the lowest chance of cross-contamination as it is hermetically sealed, making it preferable for burn wounds.
OTHER MEDICAL ITEMS
Tourniquet

This is a temporary solution to bleeding which can only be applied onto limbs. It stops bleeding by constricting circulation through pressure on the skin. This is done by wrapping a tourniquet around the upper (and sometimes lower) portion of the limb of a patient, and tightening it to ensure proper constriction and little chance of dismounting. It should be taken off the patient ASAP (within 5 to 10 minutes), else it will cause pain for the patient and eventually unconsciousness, followed by death if enough circulation has been constricted from the limb. Once a tourniquet has been removed from a patient, it will be added to the inventory of whoever removed it. It is not a disposable item.
Note that Tourniquets interfere with blood pressure and heart rate readings. If you find that you or a teammate are unable to walk or are passing out regularly, it’s possible that a tourniquet is still applied to a limb and needs removing.
Note that Tourniquets interfere with blood pressure and heart rate readings. If you find that you or a teammate are unable to walk or are passing out regularly, it’s possible that a tourniquet is still applied to a limb and needs removing.
Intravenous Drips (IV’s)

All IV’s (Saline, Plasma and Blood) restore the volume of liquid in the blood stream, as a result, blood pressure is raised for all of them. In the field saline should be the only IV deployed, as plasma and blood need refrigeration and can go bad after a period in average temperature.
Saline is a double-edged sword as it reduces blood clotting meaning that bleeding can be intensified by overuse of saline IVs. It is useful for restoring patients who have lost a little blood or stabilizing patients who are suffering from cardiac failure due to low blood pressure until MEDEVAC arrives.
Note there are different bag sizes which come in 250, 500, or 1000 ml. If available, use the correct bag size depending on how much blood has been lost from the patient. Use of any quantity of IV bags will increase blood pressure. IV treatment is not instantaneous.
Note that if the game appears desaturated and monochromatic, you will require IV treatment or risk falling unconscious.
The movement of fluids such as saline, blood, and plasma into the body are determined by a flow rate variable. This variable changes based on the size of established IVs and IOs, which smallest to largest are 20g IV, 16g IV, and 45mm IO. This variable also changes based on the heart rate of a patient as lower heart rates will mean a slower intake of fluids and in cardiac arrest, will stop entirely. Be aware establishing an IV or IO into a conscious patient will inflict pain the 16g IV causes medium pain while the Fast IO will cause severe pain, if the patient is already in pain but still conscious a Fast IO will push them past the pain thresholds and they will pass out.
However, this only applies to the 20g and 16g IV, meaning that the flow rate of the 45mm IO is not dependent on heart rate and can be used to still push fluids into a body while in cardiac arrest.
Saline is a double-edged sword as it reduces blood clotting meaning that bleeding can be intensified by overuse of saline IVs. It is useful for restoring patients who have lost a little blood or stabilizing patients who are suffering from cardiac failure due to low blood pressure until MEDEVAC arrives.
Note there are different bag sizes which come in 250, 500, or 1000 ml. If available, use the correct bag size depending on how much blood has been lost from the patient. Use of any quantity of IV bags will increase blood pressure. IV treatment is not instantaneous.
Note that if the game appears desaturated and monochromatic, you will require IV treatment or risk falling unconscious.
The movement of fluids such as saline, blood, and plasma into the body are determined by a flow rate variable. This variable changes based on the size of established IVs and IOs, which smallest to largest are 20g IV, 16g IV, and 45mm IO. This variable also changes based on the heart rate of a patient as lower heart rates will mean a slower intake of fluids and in cardiac arrest, will stop entirely. Be aware establishing an IV or IO into a conscious patient will inflict pain the 16g IV causes medium pain while the Fast IO will cause severe pain, if the patient is already in pain but still conscious a Fast IO will push them past the pain thresholds and they will pass out.
However, this only applies to the 20g and 16g IV, meaning that the flow rate of the 45mm IO is not dependent on heart rate and can be used to still push fluids into a body while in cardiac arrest.
Advanced Trauma Care Items
Surgical Kit (SK)
The surgical kit is used to completely close wounds. Each Combat Lifesaver is issued one surgical kit in the field, and it can be used an unlimited amount of times. To use it a patient must be stabilized and when the field surgery is completed his wound will be stitched up and not have a reopening chance
Personal Aid Kit (PAK)
A personal aid kit is a one hit Jesus level wonder of modern medicine. It is all-in-one medical kit designed to treat all forms of wounds. A PAK will fully heal the patient. It removes the injury and restores vitals to a stable state and reset the medical history. Clears all medication in the system. A PAK can only be used by a doctor and is typically not issued in the field during active combat. A patient must be stabilized before it can be used, and it will be removed on usage
AED X-Series
An AED X-Series is a monitor and an Automated External Defibrillator all in one. It monitors heart rate, blood pressure and oxygen saturation all in one. It can be accessed via medical menu or torso interaction.
Once the patient's vitals are being monitored it appears in the “quick view” section of the medical menu. Beeps when the patient is being monitored is the heart rate, obviously the faster the beat the faster the larger the beats per minute.
Once the patient's vitals are being monitored it appears in the “quick view” section of the medical menu. Beeps when the patient is being monitored is the heart rate, obviously the faster the beat the faster the larger the beats per minute.
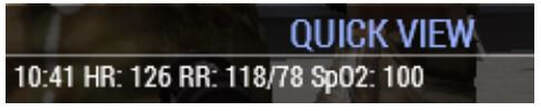
Normal vitals can be anywhere around HR: 80, RR: 120/80 mmHg, Sp02: 100%.
The defibrillator can be accessed via torso interaction or medical menu. The downside to using this item is that it generates loud noises, which may attract nearby enemies if the area is not secure. This item should only be used if the area is secure.
The defibrillator can be accessed via torso interaction or medical menu. The downside to using this item is that it generates loud noises, which may attract nearby enemies if the area is not secure. This item should only be used if the area is secure.
Pulse Oximeter
A Pulse Oximeter is similar to the AED X-Series, however it does not have a defibrillator function and does not monitor blood pressure. To use it you must select either arm then press “use pulseoximeter”. This is used by the medic as a lighter and quieter option.
Accuvac
The Accuvac is a mobile medical suction device which can be used in order to clear airways from any obstructions. If the patient is not unconscious then the device does not need to be used. This item is used via head or medical menu interaction.
Guedel Tube
The Guedel Tube is an airway securing tube, this tube lifts the tongue up so that the route of the airway is not blocked unless there are other problems like vomit and blood. It has no suction capabilities.
Stethoscope
Facilitates the diagnosis of patient (speeds it up)
King LT / Laryngealtube
The King LT is a multipurpose airway aspiration protection and securing tube. It stops vomit going into the airways. It has no suction capabilities.
Chest Seal
A chest seal is used to treat pneumothorax, it is engineered to treat, seal and reseal open chest wounds under certain circumstances.
AAT Kit
The AAT kit is an Advanced Airway Treatment single usage kit that is used to treat hemopneumothorax or tension hemopneumothorax wounds by draining fluids.
Splint
A splint is used to heals one fracture on a leg or arm.
(doesn't affect PAK time; can be applied if still bleeding!)
(doesn't affect PAK time; can be applied if still bleeding!)
Triage Card
Card that determines severity of patient's wounds. Typically used to help medics and casualty evacuation with identifying necessary levels of care.
Minimal / T1: The patient is combat effective (small bruises, scrapes, pain, controlled bleeding).
Delayed / T2: The patient is combat ineffective (bleeding controlled or minimum, broken limbs, severe weapon sway, unconscious + stable).
Immediate / T3: The patient is at an immediate risk of death (heavy bleeding, cardiac arrest, unconscious + unknown medical status).
Deceased / T4: The patient is dead. KIA.
Minimal / T1: The patient is combat effective (small bruises, scrapes, pain, controlled bleeding).
Delayed / T2: The patient is combat ineffective (bleeding controlled or minimum, broken limbs, severe weapon sway, unconscious + stable).
Immediate / T3: The patient is at an immediate risk of death (heavy bleeding, cardiac arrest, unconscious + unknown medical status).
Deceased / T4: The patient is dead. KIA.
DRUGS
AUTOINJECTORS
Morphine
Suppresses pain the patient is suffering. Blood viscosity is reduced which in turn reduces blood pressure. Do not apply Epinephrine as a result of lowered heart rate after applying Morphine. Your heart rate will return to normal in roughly 5 minutes. OD Warning: Applying too many doses of Morphine within a short span will cause Cardiac Arrest. Do not apply more than one dose of morphine within 10 minutes.
Epinephrine
Increases the heart rate of the patient. The most commonly used drug to treat ALL forms of cardiac arrest regardless of rhythm. Quick application of epinephrine in an arrest scenario is critical to the survival of any patient. Counteracts the heart rate lowering effects of Morphine & Adenosine. Epinephrine has no risk of application and while it only increases the success chance of a patient by 5 points, it offers other benefits as it stacks over time, increasing its effectiveness as the cardiac cycle goes on. Epinephrine is also the only drug that can be used to increase the success chance of a patient in non-shockable cardiac arrest.
OD Warning: Applying too many doses of Epinephrine within a short span will cause Cardiac Arrest. Do not apply more than one dose of Epinephrine within 10 minutes. After applying Epinephrine to a patient, and they keep falling unconscious, check their blood pressure.
OD Warning: Applying too many doses of Epinephrine within a short span will cause Cardiac Arrest. Do not apply more than one dose of Epinephrine within 10 minutes. After applying Epinephrine to a patient, and they keep falling unconscious, check their blood pressure.
Adenosine
Lowers the heart rate of the patient but does not remove pain. See Morphine OD warning
Atropine / ATNAA
Atropine is known primarily for two primary actions, the first is the treatment of nerve agents and certain poisons and the second is the treatment of bradycardia. Atropine may not be able to treat nerve agents (yet) but it is able to treat bradycardia created by Amiodarone and Lidocaine. Currently this medication acts like Naloxone where it simply locates the bradycardia effect in the player’s medical array and removes it, however this will become more involved over time.
PHARMACEUTICAL MEDICATIONS
Naloxone
Sold under the brand name NARCAN, Naloxone is built to combat opioid overdoses. Naloxone acts as an opioid antagonist, essentially booting opioids from their respective receptors and rendering them harmless in the body. Naloxone is primarily used to combat morphine overdoses through the simple elimination of morphine from a player’s medication array. This is done one at a time so if someone has two morphines in their array, it would take two Naloxone nasal sprays to fully eliminate morphine from the player’s system. Note that any pain that is being suppressed by the morphines will return once said morphines are removed.
Amiodarone
Amiodarone is a Class III Antiarrhythmic used most commonly for treating ventricular tachycardia. Amiodarone’s primary function is to increase the success chance of a patient under shockable cardiac arrest. When compared to the other antiarrhythmics, it is the most effective and can give a 20 point increase to a patient’s wakeup chance, however there is a downside to this as Amiodarone has a 1-in-3 chance of giving the patient bradycardia, which can decrease the standing heart rate by 15-20 points. Considering this, it is not recommended to give more than a single Amiodarone dose to a patient.
Lidocaine
Although more commonly known for its use as an anesthetic, Lidocaine has long been used as an antiarrhythmic drug for treating patients in VF/VT. Lidocaine increases the success chance of a patient in shockable cardiac arrest with less risk of bradycardia when compared to Amiodarone and in turn gives less of a boost to said success chance, standing at around 10-12 point increase. When Amiodarone fails to resuscitate a patient on the first try, Lidocaine should be the second drug a medic reaches for.
Tranexamic Acid (TXA)
Tranexamic Acid is a lysine substitute that binds to lysine receptors sites, inhibiting the breakdown of clots. Used primarily for patients who have experienced severe hemorrhaging and trauma, it is recommended by the TCCC to be used on individuals who will need significant blood transfusions in the near future. TXA should be administered as quickly as possible as it will clot open wounds and assist medics in the bandaging process. Currently this medication has no contraindications and is recommended for all unconscious patients regardless of status.
Ondansetron
Commonly known as Zofran, Ondansetron is commonly used to discourage vomiting and nausea in patients. It is recommended by the TCCC to be used to counter the vomiting that can come with the administration of certain pain management medications. Ondansetron will prevent a patient from vomiting and should be used if an airway cannot be properly established. Be advised that it will not clear any vomit currently present in the patient, just prevent additional vomit from being generated.
Norepinephrine
The first-line drug used in cases of septic shock, Norepinephrine is a vasopressor which acts on both the Alpha-1 and Beta-1/2 receptors to help with vasoconstriction and increasing cardiac output and in turn, increasing overall blood pressure. Norepinephrine will quickly increase blood pressure by 15% in a patient and will stay in a patient’s system for two minutes before clearing.
Phenylephrine
While Norepinephrine acts on both Alpha and Beta receptors, Phenylephrine is pure Alpha, focusing specifically on vasoconstriction which means its more effective at actually increasing blood pressure compared to Norepinephrine and will do so by 30%. However, the downside with this drug is that the pure alpha focus causes reflexive bradycardia in a patient meaning that while blood pressure may increase, pulse will simultaneously fall by 5-15 points while Phenylephrine is in the patient’s system.
Nitroglycerin
While Phenylephrine and Norepinephrine are focused on vasoconstriction, Nitroglycerin is instead focused on vasodilation which dilate a patient’s blood vessels and decrease their blood pressure by 15%.
OTHER
Ammonium Carbonate
Ammonium Carbonate or “smelling salts” were at one point used to recover individuals who fainted by triggering an inhalation reflex. While not currently used or recommended in any sort of medical practice, they serve to counter the nasty tendency of people getting knocked out for remarkably minor wounds. Rather than rely on the wakeup chance with Epinephrine, Ammonium Carbonate goes right to the wakeup script and will wake players up as long as they are within the stable vital threshold.
Painkillers
An analgesic or painkiller is any member of the group of drugs used to achieve analgesia, relief from pain. Analgesic drugs act in various ways on the peripheral and central nervous systems. In Arma, painkillers are used to suppress pain and have 10 uses per box, the amount used is measured by the white line on the left hand side. It is weaker than morphine and does not lower heart rate however it increases blood pressure. Painkillers can be found in the magazine section.
TRAUMA CARE
Trauma management can be simplified into the following for Arma:
Bleeding
Simplified is the Patient Bleeding.
Breathing
Include breathing and Oxygen saturation
Beating
Includes pulse and blood volume
Bleeding
Simplified is the Patient Bleeding.
Breathing
Include breathing and Oxygen saturation
Beating
Includes pulse and blood volume
BLEEDING
The priority in combat medicine is always to keep the blood inside the body. Bleeding control and management is more important than anything else because without it all other efforts will be wasted.
Each limb on the body can receive different types of injury. Each injury has a different level of pain and bleeding that it will inflict. Each injury type also has a set of treatment procedures that are best suited for it - these will be laid out in the subsequent chapter about rendering aid.
Abrasion
Also known as a scrape. Occurs when skin is rubbed away against a rough surface.
• Caused by falling and lesser vehicle crashes.
• Causes light pain and slow bleeding.
• Caused by falling and lesser vehicle crashes.
• Causes light pain and slow bleeding.
Avulsion
Occurs when body matter is forcibly pulled away, such as the loss of a permanent tooth or an ear lobe. Explosions, gunshots and animal bites may cause avulsions.
• Caused by shrapnel from explosions, vehicle crashes, bullets, backblast.
• Causes extremely high pain and extremely fast bleeding
• Caused by shrapnel from explosions, vehicle crashes, bullets, backblast.
• Causes extremely high pain and extremely fast bleeding
Burn
Occurs when skin or body parts are damaged by extreme heat, flame, contact with heated objects, or chemicals.
• Caused by explosions, rope burns, back blast, shells and heat related injuries (e.g. getting struck by a incendiary device or getting in contact with a vehicle on fire)
• Causes extremely high pain and slow bleeding
• Caused by explosions, rope burns, back blast, shells and heat related injuries (e.g. getting struck by a incendiary device or getting in contact with a vehicle on fire)
• Causes extremely high pain and slow bleeding
Contusion
Also called bruises, these are the result of a forceful trauma that injure the internal structure without breaking the skin. Blows to the chest, abdomen, or head with a blunt instrument (e.g. a football or a fist) can cause contusions.
• Caused by backblast, lesser vehicle crashes, falling, and ricochets.
• Causes light pain & limited bleeding.
• Caused by backblast, lesser vehicle crashes, falling, and ricochets.
• Causes light pain & limited bleeding.
Crush
Occurs when a heavy object falls onto a person, splitting the skin and shattering or tearing underlying structures.
• Caused by falling, physics related occurrences, and vehicle crashes.
• Causes light pain and slow bleeding.
• Caused by falling, physics related occurrences, and vehicle crashes.
• Causes light pain and slow bleeding.
Cut
Occurs when sharp material slices body tissue, leaving even edges, they may be as minimal as a paper cut or as significant as a surgical incision.
• Caused by vehicle crashes, shrapnel, and backblast.
• Causes light pain and with a slow bleed rate
• Caused by vehicle crashes, shrapnel, and backblast.
• Causes light pain and with a slow bleed rate
Velocity
Occurs when an external object enters the body at high speed.
• Caused by shrapnel and bullets.
• Causes lots of pain and medium bleed rate
• Caused by shrapnel and bullets.
• Causes lots of pain and medium bleed rate
Puncture
Deep, narrow wounds produced by sharp objects such as nails, knives, and broken glass
• Caused by shrapnel.
• Causes light pain and slow bleeding.
• Caused by shrapnel.
• Causes light pain and slow bleeding.
BREATHING
Breathing is the second most important thing, if the blood is not carrying oxygen this service has no purpose.
Airway & Respiration Control
Airway management is the process of ensuring that:
• There is an open pathway between a patient’s lungs and the outside world, and, the lungs are able to aspirate
• There is an open pathway between a patient’s lungs and the outside world, and, the lungs are able to aspirate
To check the patient’s airways you must open the medical menu and select the head, here we get an option to “check airways” in the section of “examine patient” .


If the patient needs no airway management then the normal treatment procedures can be followed. In the case where airway management is needed it will say “airway management needed” and thus the first responder must reference the following.
Head Turning
In the case of an occluded airway (symptoms of puking) you must either use an Accuvac or use the Head Turning treatment. The Head Turning has a smaller chance of success (35% default) compared to the Accuvacs 100%.
Head Overstretch / Hyperextending Head
In the case of a collapsed airway/lung you should use a nasopharyngeal airway device (King LT or Guedel Tube) however if you are lacking any of the tubes you should overstretch the head. This treatment, if successful, will increase the blood oxygen saturation (SPO2).
Blood Oxygen Saturation
Blood Oxygen Saturation is measured in SP02 values, they signify from a 100 to 0 from the patients values. From the moment the saturation hits 5% the patient will die. If the airway is secured either by overstretching the head or insertion of a NPA the value of the blood oxygen saturation should increase. If the saturation is lower than 70% then the patient will be unconscious.
If the saturation is lower than 90% then the patient will be unconscious.
The moment the saturation hits 10% the patient will die.
If the saturation is lower than 90% then the patient will be unconscious.
The moment the saturation hits 10% the patient will die.
Pneumothorax
Pneumothorax is a medical event where the lung is damaged and leaks air into the chest cavity damaging lungs over a prolonged time.
In order to treat Pneumothorax medics will have an option to use a chest seal under the chest section in the ace medical menu. It can be spotted by seeing the blood oxygen saturation levels dropping quickly, it is also worth noting that using an NPA on a patient will not work if Pneumothorax is diagnosed (this is how you can tell if a patient has it).
In order to treat Pneumothorax medics will have an option to use a chest seal under the chest section in the ace medical menu. It can be spotted by seeing the blood oxygen saturation levels dropping quickly, it is also worth noting that using an NPA on a patient will not work if Pneumothorax is diagnosed (this is how you can tell if a patient has it).
Tension Pneumothorax
A tension pneumothorax is a life-threatening condition that develops when air is trapped in the pleural cavity under positive pressure, displacing mediastinal structures and compromising cardiopulmonary function.
In order to treat tension pneumothorax medics will have an option to use an AAT Kit under the chest section in the ace medical menu.
In order to treat tension pneumothorax medics will have an option to use an AAT Kit under the chest section in the ace medical menu.
Hemothorax
The accumulation of blood in the pleural cavity (the space between the lungs and the walls of the chest)
In order to treat a Hemothorax medics will have an option to use an AAT Kit under the chest section in the ace medical menu.
In order to treat a Hemothorax medics will have an option to use an AAT Kit under the chest section in the ace medical menu.
BEATING
Blood Pressure
Systolic pressure refers to the amount of pressure in your arteries during contraction of your heart muscle.
Diastolic pressure refers to your blood pressure when your heart muscle is between beats.
Blood pressure is affected by the amount of lost blood, IV’s, tourniquets and medications from autoinjectors. Only combat lifesavers can view blood pressure details of themselves and of patients.
Note that the way to phrase blood pressure is systolic over diastolic, with the former being the top number and the latter being the bottom. E.g, a normal blood pressure would be 100 over 160.
Diastolic pressure refers to your blood pressure when your heart muscle is between beats.
Blood pressure is affected by the amount of lost blood, IV’s, tourniquets and medications from autoinjectors. Only combat lifesavers can view blood pressure details of themselves and of patients.
Note that the way to phrase blood pressure is systolic over diastolic, with the former being the top number and the latter being the bottom. E.g, a normal blood pressure would be 100 over 160.
Heart Rate
This is affected by the amount of lost blood and medications. You can check you or a patient’s heart rate by using ACE interaction and looking at a limb, then use the option to check heart rate. Combat Lifesavers will be granted more detailed information, whereas a non-CLS will see “You find a normal heart rate” or something similar.
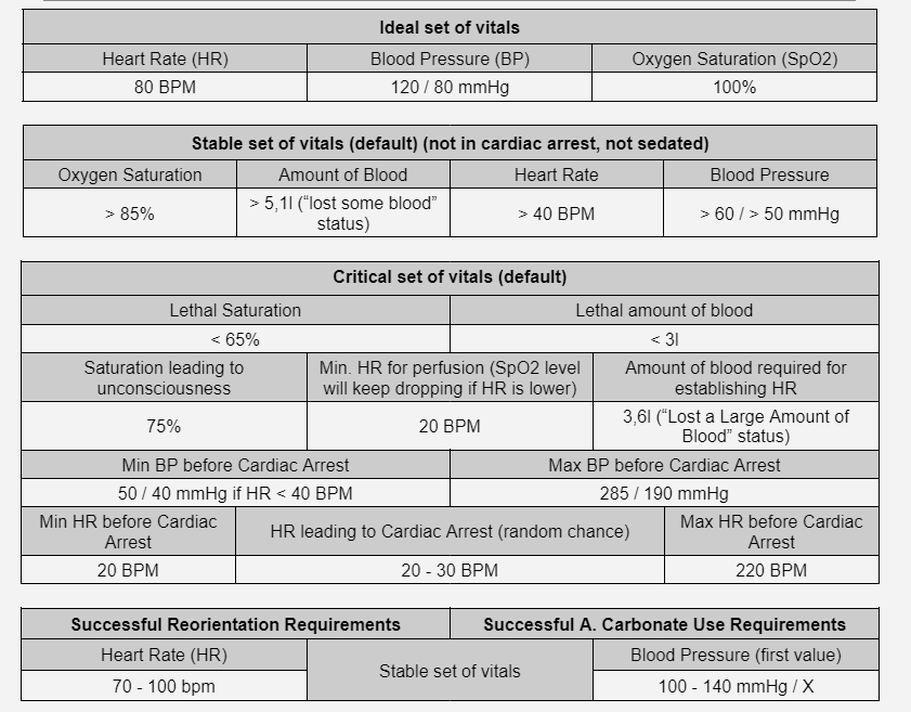
Cardiac Arrest
This occurs under the following circumstances:
• Heart Rate is <20
• Heart rate is >200
• Systolic blood pressure is >260
• Diastolic blood pressure is <40 and the heart rate >190
• Systolic blood pressure is >145 and the heart rate is >150
The latter points appear complicated, however they should be viewed as the worst possible results for blood pressure and heart rate combined. Apply CPR in case of cardiac arrest.
There are multiple medications that are built specifically to interact with the cardiac arrest system that now has two classifications of arrest rhythms, shockable (VF/PVT) and non-shockable (Asystole). As the names suggest, shockable rhythms can be treated with either the AED or AED-X while the non-shockable rhythms can only be treated through manual CPR. Shockable rhythms can also be treated with Epinephrine, Lidocaine, and Amiodarone while non-shockable rhythms can only be treated with Epinephrine.
The determination for which rhythm a patient will fall into is made on the first CPR or Analyze Rhythm action performed on a patient. If at the time a patient has lost a fatal amount of blood, then they are almost guaranteed to fall into asystole and if they have more than that, then they will fall into VF/PVT. While this may seem gamey, it is done with the intention to emphasise quick recognition and response to cardiac arrest. Patients who are put into the cardiac arrest algorithm the quickest will be the easiest for medics to treat and the first ones to get back in the fight.
• Heart Rate is <20
• Heart rate is >200
• Systolic blood pressure is >260
• Diastolic blood pressure is <40 and the heart rate >190
• Systolic blood pressure is >145 and the heart rate is >150
The latter points appear complicated, however they should be viewed as the worst possible results for blood pressure and heart rate combined. Apply CPR in case of cardiac arrest.
There are multiple medications that are built specifically to interact with the cardiac arrest system that now has two classifications of arrest rhythms, shockable (VF/PVT) and non-shockable (Asystole). As the names suggest, shockable rhythms can be treated with either the AED or AED-X while the non-shockable rhythms can only be treated through manual CPR. Shockable rhythms can also be treated with Epinephrine, Lidocaine, and Amiodarone while non-shockable rhythms can only be treated with Epinephrine.
The determination for which rhythm a patient will fall into is made on the first CPR or Analyze Rhythm action performed on a patient. If at the time a patient has lost a fatal amount of blood, then they are almost guaranteed to fall into asystole and if they have more than that, then they will fall into VF/PVT. While this may seem gamey, it is done with the intention to emphasise quick recognition and response to cardiac arrest. Patients who are put into the cardiac arrest algorithm the quickest will be the easiest for medics to treat and the first ones to get back in the fight.

This is a basic cardiac arrest algorithm. once you walk through it. Once cardiac arrest has been entered, the first priority is attaching a defibrillator to determine if the patient’s rhythm is shockable or not. Depending on what you are told, it breaks down into two patterns, the VF/PVT and Asystole patterns. VF/PVT is based on the use of AEDs to deliver shocks to the patient and administer our three main antiarrhythmics. If at any time ROSC (return of spontaneous circulation) is achieved, the pattern stops and we move into post-arrest care. Note that currently VF/PVT cannot devolve into Asystole so if a patient is in VF/PVF, they are staying there until they are out of cardiac arrest.
Asystole on the other hand is based on manual CPR and Epinephrine with periodic rhythm checks every three rounds of CPR to determine if we have moved out of Asystole and into VF/PVT. While this pattern suggests that Asystole can only move to VF/PVT and nothing else, it should be noted that Asystole also has a chance to move right into ROSC at which time the pattern stops and the treating medic will conduct post-arrest care. Also be advised even if CPR succeeds, failure to get a patient into the “Lost a Large Amount of Blood” category will trigger another asystole check and will push the patient back into asystole. Medics should also remember that if no defibrillation equipment is available, they should treat all cardiac arrest cases as if they are in Asystole as while the VF/PVT pattern and the medications Lidocaine and Amiodarone only work for shockable rhythms, the Asystole pattern works for all rhythms.
Asystole on the other hand is based on manual CPR and Epinephrine with periodic rhythm checks every three rounds of CPR to determine if we have moved out of Asystole and into VF/PVT. While this pattern suggests that Asystole can only move to VF/PVT and nothing else, it should be noted that Asystole also has a chance to move right into ROSC at which time the pattern stops and the treating medic will conduct post-arrest care. Also be advised even if CPR succeeds, failure to get a patient into the “Lost a Large Amount of Blood” category will trigger another asystole check and will push the patient back into asystole. Medics should also remember that if no defibrillation equipment is available, they should treat all cardiac arrest cases as if they are in Asystole as while the VF/PVT pattern and the medications Lidocaine and Amiodarone only work for shockable rhythms, the Asystole pattern works for all rhythms.
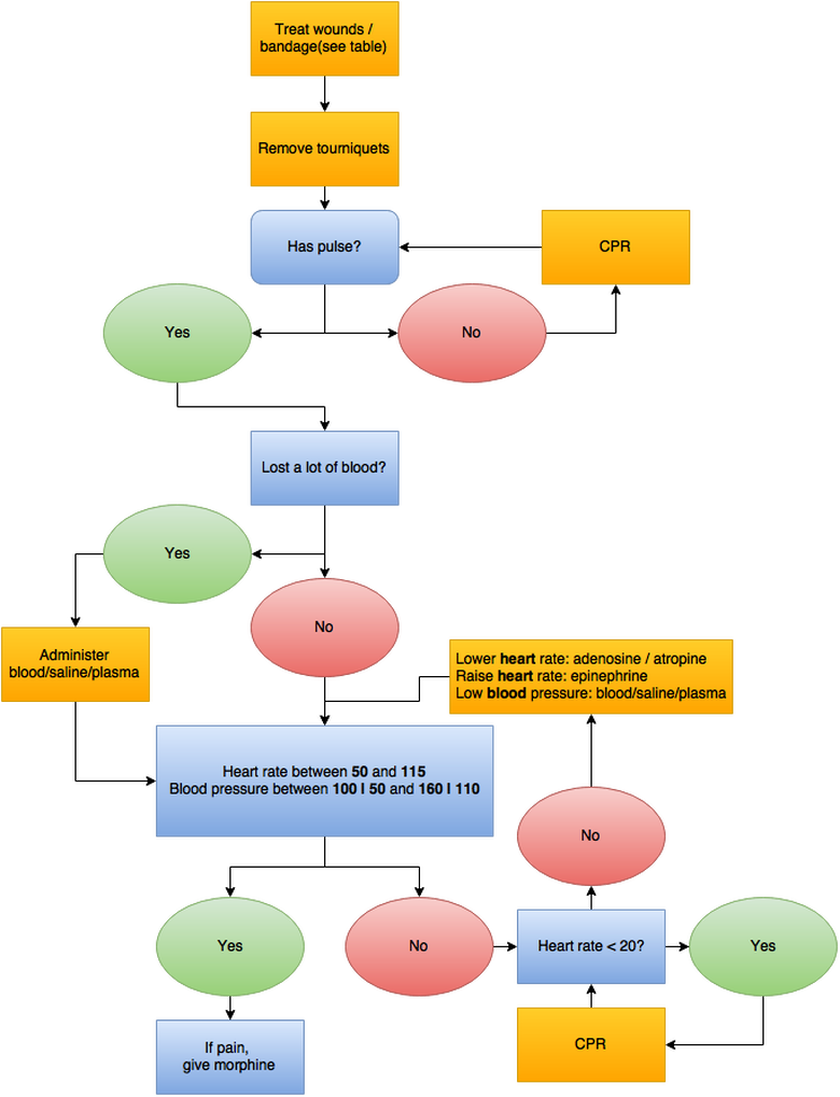
Cardiopulmonary Resuscitation (CPR)
CPR is an emergency procedure that combines chest compressions in an effort to manually preserve intact brain function until further measures are taken to restore spontaneous blood circulation and breathing in a person who is in cardiac arrest.
Used to keep a player alive if they have a critically low heart rate. The patient’s heart rate will be ~25 upon success. From here, provided the patient is not wounded, you can use Epinephrine to increase their heart rate and bring them back to consciousness.
NOTE: If not using KAT Pharmacy, follow the chart below.
Used to keep a player alive if they have a critically low heart rate. The patient’s heart rate will be ~25 upon success. From here, provided the patient is not wounded, you can use Epinephrine to increase their heart rate and bring them back to consciousness.
NOTE: If not using KAT Pharmacy, follow the chart below.
Circulation
Flow Rate System: The movement of fluids such as saline, blood, and plasma into the body are now determined by a flow rate variable. This variable changes based on the size of established IVs and IOs, which smallest to largest are 20g IV, 16g IV, and 45mm IO. This variable also changes based on the heart rate of a patient as lower heart rates will mean a slower intake of fluids and in cardiac arrest, will stop entirely.
However, this only applies to the 20g and 16g IV, meaning that the flow rate of the 45mm IO is not dependent on heart rate and can be used to still push fluids into a body while in cardiac arrest. (This decision is based on gameplay considerations as to give players a reason to pick different sized IVs and IOs. Very subject to change in the near future).
However, this only applies to the 20g and 16g IV, meaning that the flow rate of the 45mm IO is not dependent on heart rate and can be used to still push fluids into a body while in cardiac arrest. (This decision is based on gameplay considerations as to give players a reason to pick different sized IVs and IOs. Very subject to change in the near future).
Blood Types
Blood types are determined by the presence or absence of certain antigens – substances that can trigger an immune response if they are foreign to the body. Since some antigens can trigger a patient's immune system to attack the transfused blood, safe blood transfusions depend on careful blood typing and cross-matching.
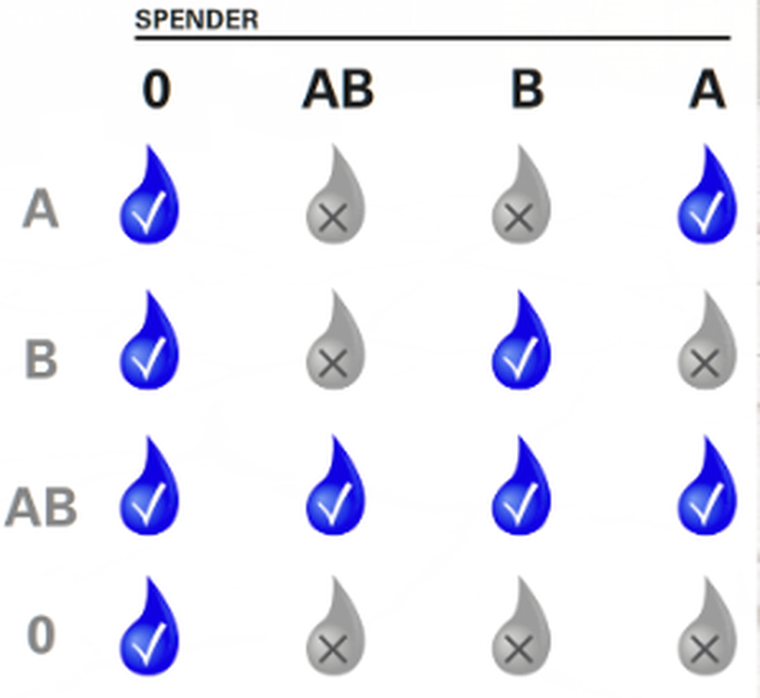
In order to check the patient's blood type, the combat lifesaver must open up the medical menu and select the head and check his dogtags. On this dogtag there will be the blood group that the patient has. It is vital that blood is never given on the field and should only be given at a combat hospital or casualty collection point if feasible. If blood is to be given, it is important that the recipient is receiving blood that is compatible with his blood type, giving the wrong type of blood is fatal, the only way to treat wrongly given blood is to give saline to the patient immediately afterwards. Symptoms of wrongly given blood can be blurred/doubled vision (first symptom) for the patient and a faster heart rate.
Revive
The revive system lets you bring downed units back up. Upon receiving a deadly amount of damage a unit will fall unconscious. In that time a medic will need to treat them to bring them back up.
Unconsciousness happens when one of the following is met:
• Pain threshold is reached
• Low Blood pressure
• Cardiac Arrest.
• Oxygen saturation below 70%
Someone can not recover from unconsciousness till the underlying factor has been resolved.
Death happens if one of the following happens.
• Nonexistent: 0 - 20 systolic.
• Oxygen saturation below 5%
• The Cardiac Arrest timer runs out, the base timer is 300 seconds (5 minutes), this can be extended to a max of 3600 seconds (60 minutes) with CPR each usage will extend the timer by 120 seconds.
• Pain threshold is reached
• Low Blood pressure
• Cardiac Arrest.
• Oxygen saturation below 70%
Someone can not recover from unconsciousness till the underlying factor has been resolved.
Death happens if one of the following happens.
• Nonexistent: 0 - 20 systolic.
• Oxygen saturation below 5%
• The Cardiac Arrest timer runs out, the base timer is 300 seconds (5 minutes), this can be extended to a max of 3600 seconds (60 minutes) with CPR each usage will extend the timer by 120 seconds.
TACTICAL COMBAT CASUALTY CARE
Tactical Combat Casualty Care (TCCC or TC3) is the standard of care in Prehospital Battlefield Medicine. Tactical Combat Casualty Care (TCCC) is intended to treat potentially preventable causes of death on the battlefield, but acknowledges that application of these treatments may place the provider and even the mission in jeopardy if performed at the wrong time. Therefore, TCCC classifies the tactical situation with respect to health care provision into 3 phases (care under fire, tactical field care and tactical evacuation) and only permits certain interventions to be performed in specific phases based on the danger to the provider and casualty.
The TCCC Guidelines are routinely updated and published by the Committee on Tactical Combat Casualty Care (CoTCCC), a component of the Joint Trauma System (JTS). TCCC was designed in the mid-'90s for the Special Operations medical community. Originally a Naval Special Warfare and USSOCOM Medical Research & Development initiative, TCCC developed battlefield appropriate and evidence-based casualty care based on injury patterns of previous conflicts. The original TCCC concept and guidelines were published in a Military Medicine Supplement in 1996. The primary intent of TCCC is to reduce preventable combat death through a means that allows a unit to complete its mission while providing the best possible care for casualties. Now it is a DOD course, conducted by NAEMT. TCCC or similar standards are used by most allied countries.
In the many years that coalition forces have been involved in sustained combat operations in Afghanistan and Iraq, more than 400,000 have been injured and more than 240,000 have been killed, including civilians and aid workers. As a result, substantial experience was gained delivering TCCC to wounded persons on the battlefield. The purpose of this paper is to review the principles of TCCC and some of the lessons learned about battlefield trauma care during conflict.
The TCCC Guidelines are routinely updated and published by the Committee on Tactical Combat Casualty Care (CoTCCC), a component of the Joint Trauma System (JTS). TCCC was designed in the mid-'90s for the Special Operations medical community. Originally a Naval Special Warfare and USSOCOM Medical Research & Development initiative, TCCC developed battlefield appropriate and evidence-based casualty care based on injury patterns of previous conflicts. The original TCCC concept and guidelines were published in a Military Medicine Supplement in 1996. The primary intent of TCCC is to reduce preventable combat death through a means that allows a unit to complete its mission while providing the best possible care for casualties. Now it is a DOD course, conducted by NAEMT. TCCC or similar standards are used by most allied countries.
In the many years that coalition forces have been involved in sustained combat operations in Afghanistan and Iraq, more than 400,000 have been injured and more than 240,000 have been killed, including civilians and aid workers. As a result, substantial experience was gained delivering TCCC to wounded persons on the battlefield. The purpose of this paper is to review the principles of TCCC and some of the lessons learned about battlefield trauma care during conflict.
Objectives of TCCC
The three objectives of TCCC are to provide lifesaving care to the injured combatant, to limit the risk of further casualties, and to help the unit achieve mission success.
- Treat injured combatants
- Limit the risk of further casualties
- Achieve mission success
Phases of Care
In TCCC prehospital battlefield care is divided into 3 phases:
• Care under fire
• Tactical field care
• Tactical evacuation care (TACEVAC).
These are united together under the guiding principle of “providing the right medicine at the right time,” which is divided into phases of care.
• Care under fire
• Tactical field care
• Tactical evacuation care (TACEVAC).
These are united together under the guiding principle of “providing the right medicine at the right time,” which is divided into phases of care.
Care Under Fire (CUF)
CUF is characterized as the care rendered to a casualty while still under effective fire. In most situations during active combat, both the casualty and the care provider are in danger from enemy fire and may or may not be behind adequate cover and may need to contribute to the firefight. It is commonly said that “the best battlefield medicine is fire superiority;” therefore, winning the firefight and establishing a secure cordon within which to operate is the primary objective during CUF. In this case, the first action is to return fire and take cover as fire superiority over the enemy is the best medicine to include the casualty remaining engaged if able. As an enemy is suppressed, casualties can move or be moved to more secure positions.
The only medical treatment rendered in CUF is stopping life-threatening hemorrhage (bleeding). TCCC actively endorses and recommends the early and immediate use of tourniquets to control massive external hemorrhage of limbs and establishing an recovery position for airway obstruction should the tactical situation allow for it. All other treatment should be delayed until the casualty can be moved to a more secure and covered position and transitioned to tactical field care.
The only medical treatment rendered in CUF is stopping life-threatening hemorrhage (bleeding). TCCC actively endorses and recommends the early and immediate use of tourniquets to control massive external hemorrhage of limbs and establishing an recovery position for airway obstruction should the tactical situation allow for it. All other treatment should be delayed until the casualty can be moved to a more secure and covered position and transitioned to tactical field care.
There is no Medicine in a firefight.
You should not attempt to render aid to a casualty until the friendly force has obtained fire superiority.
Failure to ensure that the friendly force hold fire superiority can lead to a multiplication of casualties as first responders become injured.
Care under Fire is the actions undertaken by the squadmates of the injured personnel when a casualty is first injured. This phase revolves solely around bleeding control.
You should not attempt to render aid to a casualty until the friendly force has obtained fire superiority.
Failure to ensure that the friendly force hold fire superiority can lead to a multiplication of casualties as first responders become injured.
Care under Fire is the actions undertaken by the squadmates of the injured personnel when a casualty is first injured. This phase revolves solely around bleeding control.
Tactical Field Care (TFC)
TFC is care rendered by first responders or prehospital medical personnel (primarily medics, corpsman, and pararescuemen) while still in the tactical environment. Tactical field care is rendered once the casualty, the care provider and their unit are no longer under effective hostile fire. It also applies to situations in which an injury has occurred on a mission, but in which hostile fire has not yet been encountered. Equipment is limited to that carried by the care provider, casualty and their team. It is during this phase of care that the bulk of the TCCC interventions are performed. TFC is focused on assessment and management using the MARCH acronym.
Continued assessment and management in TFC includes treating penetrating eye trauma, assessing for traumatic brain injury or head injuries, treating burns, splinting fractures, and dressing non-life-threatening wounds. TCCC promotes the early and aggressive use of analgesia (pain management) on the battlefield through the administration of Ketamine and/or Oral Tranmuccossal Fentanyl for casualties with moderate to severe pain. TCCC also promotes the early administration oral and intravenous or intramuscular antibiotics. The remainder of TFC care is dedicated is reassessment of injuries and interventions, documentation of care, communicating with tactical leadership and evacuation assets. TFC culminates with packaging a casualty for evacuation and then evacuating by available air, ground, or maritime assets.
- Massive hemorrhage is managed through the use of tourniquets, hemostatic dressings, junctional devices, and pressure dressings.
- The Airway is managed by rapid and aggressive opening of the airway to include cricothyroidotomy for difficult airways.
- Respirations and breathing is managed by the assessment for tension pneumothorax and aggressive use of needle decompression devices to relieve tension and improve breathing.
- Circulation impairment is assessed and managed through the initiation of intravenous access followed up by administration of tranexamic acid (TXA) if indicated, and a fluid resuscitation challenge using the principles of hypotensive resuscitation. TCCC promotes the early and far forward use of blood and blood products if available over the use colloids and discourages the administration of crystalloids such as normal saline (sodium chloride).
- Hypothermia prevention is an early and critical intervention to keep a traumatized casualty warm regardless of the operational environment.
Continued assessment and management in TFC includes treating penetrating eye trauma, assessing for traumatic brain injury or head injuries, treating burns, splinting fractures, and dressing non-life-threatening wounds. TCCC promotes the early and aggressive use of analgesia (pain management) on the battlefield through the administration of Ketamine and/or Oral Tranmuccossal Fentanyl for casualties with moderate to severe pain. TCCC also promotes the early administration oral and intravenous or intramuscular antibiotics. The remainder of TFC care is dedicated is reassessment of injuries and interventions, documentation of care, communicating with tactical leadership and evacuation assets. TFC culminates with packaging a casualty for evacuation and then evacuating by available air, ground, or maritime assets.
MARCHE
In our organization, the MARCHE protocol is followed. Its goal is to address the potentially preventable causes of death seen in modern warfare. Therefore, the algorithm prioritizes the treatment of exsanguinating hemorrhage with a combination of direct/indirect pressure, tourniquets and packing with hemostatic agents. Once massive hemorrhage is initially managed, combat lifesavers progress to airway and breathing issues. They can insert nasopharyngeal airways, but are also trained to perform surgical cricothryotomies for patients with massive facial trauma. For breathing, combat lifesavers can perform needle decompression of tension pneumothoraces and apply dressings to sucking chest wounds. After airway and breathing, combat lifesavers return to their “circulation” by treating hypovolemic shock through careful fluid administration, guided by field-appropriate permissive hypotension responses, via an intravenous or intraosseous route. They also assess and splint pelvic and long-bone fractures during this phase. Combat Lifesavers are taught to be cognizant of the possibility of severe brain injury and to prevent hypothermia. They can administer antibiotics for all wounds and narcotics for pain relief. Combat lifesavers are also taught the appropriateness of providing care based on the tactical situation. In an effort to accomplish this, TCCC interventions are carried out during distinct conditions, termed “phases of care.” The MARCHE Algorithm is as follows.
1. Massive hemorrhage control
(tourniquets and hemostatic dressings, prioritisation of wounds)
2. Airway management
(including surgical cricothyroidotomy/emergency airway management)
3. Respiratory management
(occlusive dressings for open pneumothoraces and needle decompression for tension pneumothoraces)
4. Circulation (TBIF)
• Tourniquet assessment and removal
• Bleeding, Blood Pressure & Heart Rate control
• Intravenous/intraosseous access
• Fluid resuscitation (HSD/hypertonic saline/dextran as a volume expander)
• Use of Autoinjectors
5. Hypothermia, Head injury & Eye injury
6. Everything else (M-PHAAT-D)
• Monitoring
• Pain
• Head to toe final assessment
• Address all wounds
• Antibiotics
• Tactical evacuation preparation
• Documentation of care
(tourniquets and hemostatic dressings, prioritisation of wounds)
2. Airway management
(including surgical cricothyroidotomy/emergency airway management)
3. Respiratory management
(occlusive dressings for open pneumothoraces and needle decompression for tension pneumothoraces)
4. Circulation (TBIF)
• Tourniquet assessment and removal
• Bleeding, Blood Pressure & Heart Rate control
• Intravenous/intraosseous access
• Fluid resuscitation (HSD/hypertonic saline/dextran as a volume expander)
• Use of Autoinjectors
5. Hypothermia, Head injury & Eye injury
6. Everything else (M-PHAAT-D)
• Monitoring
• Pain
• Head to toe final assessment
• Address all wounds
• Antibiotics
• Tactical evacuation preparation
• Documentation of care
Tactical Evacuation Care (TACEVAC)
Tactical evacuation care is care rendered during evacuation to a medical treatment facility, usually on a vehicle, aircraft or boat. This may include dedicated personnel and prepositioned equipment on these platforms. TACEVAC care encompasses the same assessment and management included in TFC with additional focus on advanced procedures that can be initiated when en route to a medical treatment facility. The caveat of TACEVAC is the evacuation means and care may or may not be dedicated medical platforms such as a MEDEVAC helicopter. TACEVAC can also include the evacuation of casualties on available non-medical assets and the provision of care in such circumstances.
In a hostile environment it is important to note that these phases are fluid; the first responders may find themselves in a situation where the phases are dynamic, and they must always be ready to adapt.
• Monitoring of patient
• Head to toe final assessment of patient
• Address any and all final wounds
• Additional antibiotics & pain management
• Tactical evacuation preparation (TC3 card)
• Documentation of care
• MEDEVAC/CASEVAC
In a hostile environment it is important to note that these phases are fluid; the first responders may find themselves in a situation where the phases are dynamic, and they must always be ready to adapt.
• Monitoring of patient
• Head to toe final assessment of patient
• Address any and all final wounds
• Additional antibiotics & pain management
• Tactical evacuation preparation (TC3 card)
• Documentation of care
• MEDEVAC/CASEVAC
Medical Evacuation 9-Line
Initial Contact:
"Alpha, this is Bravo, standby for 9-liner, over"
LINE 1 - Grid (MANDATORY READBACK)
Example: “115 373”
LINE 2 - Callsign & Frequency:
“Callsign & frequency remains the same”
LINE 3 - Precedence:
“Routine, Priority, or Urgent”
LINE 4 - Special Equipment Needed:
Ex: “Surgical equipment, x6 mags of 5.56, 4 MREs” (Be specific)
LINE 5 - Patients by type (MANDATORY READBACK):
(Ambulatory or Litter)
Ex: “3x Ambulatory and 4x Litter”
(Litter patients cannot walk, ambulatory patients can walk.)
LINE 6 - Security of Pickup sight:
Ex: “360 degree security on the LZ, little resistance from the south”
LINE 7 - Method of marking (MANDATORY READBACK):
(Smoke, Pyro, Other. Never say the color of smoke or marking unless defined by OPORD or SOP)
LINE 8 - Number of Patients nationality:
• US MIL (U.S. Military),
• FOREIGN MIL (Foreign Military),
• EPW (Enemy Prisoner of War),
• US CIV (U.S. Civilian),
• FOREIGN CIV (Foreign Civilian).
LINE 9 CBRN Threat or Terrain Description:
“No known Contaminants / Terrain is an open field surrounded by hills”
(Receiver: “Be advised, helo is en-route to your pos, ETA 20 mikes”)
"Alpha, this is Bravo, standby for 9-liner, over"
LINE 1 - Grid (MANDATORY READBACK)
Example: “115 373”
LINE 2 - Callsign & Frequency:
“Callsign & frequency remains the same”
LINE 3 - Precedence:
“Routine, Priority, or Urgent”
LINE 4 - Special Equipment Needed:
Ex: “Surgical equipment, x6 mags of 5.56, 4 MREs” (Be specific)
LINE 5 - Patients by type (MANDATORY READBACK):
(Ambulatory or Litter)
Ex: “3x Ambulatory and 4x Litter”
(Litter patients cannot walk, ambulatory patients can walk.)
LINE 6 - Security of Pickup sight:
Ex: “360 degree security on the LZ, little resistance from the south”
LINE 7 - Method of marking (MANDATORY READBACK):
(Smoke, Pyro, Other. Never say the color of smoke or marking unless defined by OPORD or SOP)
LINE 8 - Number of Patients nationality:
• US MIL (U.S. Military),
• FOREIGN MIL (Foreign Military),
• EPW (Enemy Prisoner of War),
• US CIV (U.S. Civilian),
• FOREIGN CIV (Foreign Civilian).
LINE 9 CBRN Threat or Terrain Description:
“No known Contaminants / Terrain is an open field surrounded by hills”
(Receiver: “Be advised, helo is en-route to your pos, ETA 20 mikes”)
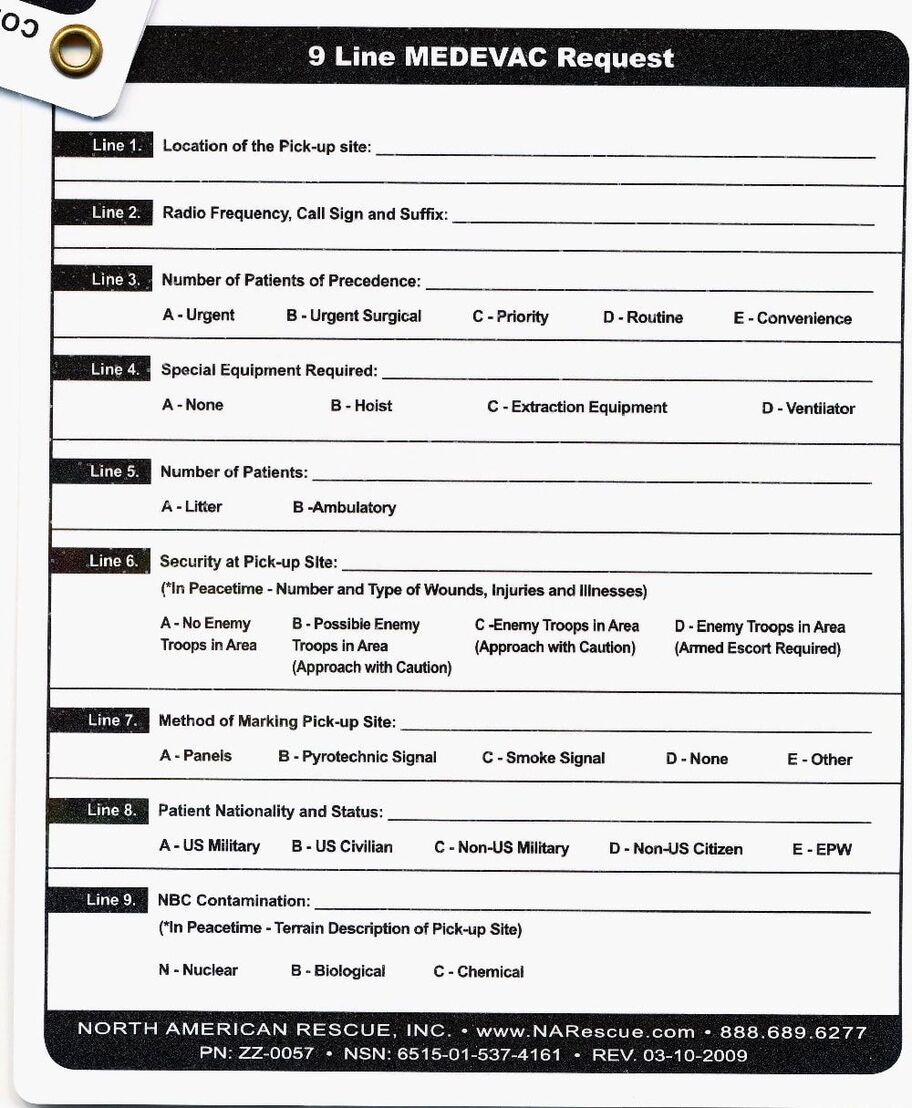
ZMIST Report
Initial Contact:
"Alpha, this is Bravo, standby for ZMIST, over"
(If you have more than one patient, give a ZMIST for each patient.)
Patient #:
(Patient one or more)
Zap number:
(First and Last initial, last 4 of tag number, add unit or unit type if patient represents a specific unit, blood type)
Ex: “MR2234 1IR, ONEG”
Mechanism of Injury:
(What caused the injury)
Ex: “Enemy small arms fire”
Injury sustained:
(Fall, MVA, GSW, RPG, IED/Mine
or
Abrasion, Avulsion, Contusion, Crush, Cut, Laceration, Velocity, Puncture.)
Ex: “3x Velocity wounds to the chest, 2x lacerations to the legs”
Symptoms:
Ex: “Low blood pressure, unconscious, excessive bleeding”
Treatment rendered:
Ex: Elastic bandages & quicklot applied to chest, x1 tourniquet applied to left leg.
(You: “How copy on all?”)
(Receiver: “Roger, solid copy. Patching you into the helo now for the LZ brief”)
"Alpha, this is Bravo, standby for ZMIST, over"
(If you have more than one patient, give a ZMIST for each patient.)
Patient #:
(Patient one or more)
Zap number:
(First and Last initial, last 4 of tag number, add unit or unit type if patient represents a specific unit, blood type)
Ex: “MR2234 1IR, ONEG”
Mechanism of Injury:
(What caused the injury)
Ex: “Enemy small arms fire”
Injury sustained:
(Fall, MVA, GSW, RPG, IED/Mine
or
Abrasion, Avulsion, Contusion, Crush, Cut, Laceration, Velocity, Puncture.)
Ex: “3x Velocity wounds to the chest, 2x lacerations to the legs”
Symptoms:
Ex: “Low blood pressure, unconscious, excessive bleeding”
Treatment rendered:
Ex: Elastic bandages & quicklot applied to chest, x1 tourniquet applied to left leg.
(You: “How copy on all?”)
(Receiver: “Roger, solid copy. Patching you into the helo now for the LZ brief”)
