A CCP - Casualty Collection Point is an ad-hoc glorified First Aid Station, often in a hostile environment and born out of a need to provide medical care to troops on the battlefield before taking them to the next higher echelon of care.
CCPs are usually platoon to company sized but in some cases may be squad sized.
A CCP is used for the assembly, triage (medical sorting in order of severity), medical stabilization and subsequent evacuation of casualties,
2 types of CCPs exist:
• Hasty
• Deliberate
Hasty - are not planned ahead of time and are dictated by the circumstances
Deliberate - ALL planned operations should have CCPs and other medical preparations (AXP - Ambulance eXchange Point) incorporated into each phase of the operation
A CCP is used for the assembly, triage (medical sorting in order of severity), medical stabilization and subsequent evacuation of casualties,
2 types of CCPs exist:
• Hasty
• Deliberate
Hasty - are not planned ahead of time and are dictated by the circumstances
Deliberate - ALL planned operations should have CCPs and other medical preparations (AXP - Ambulance eXchange Point) incorporated into each phase of the operation
Shape
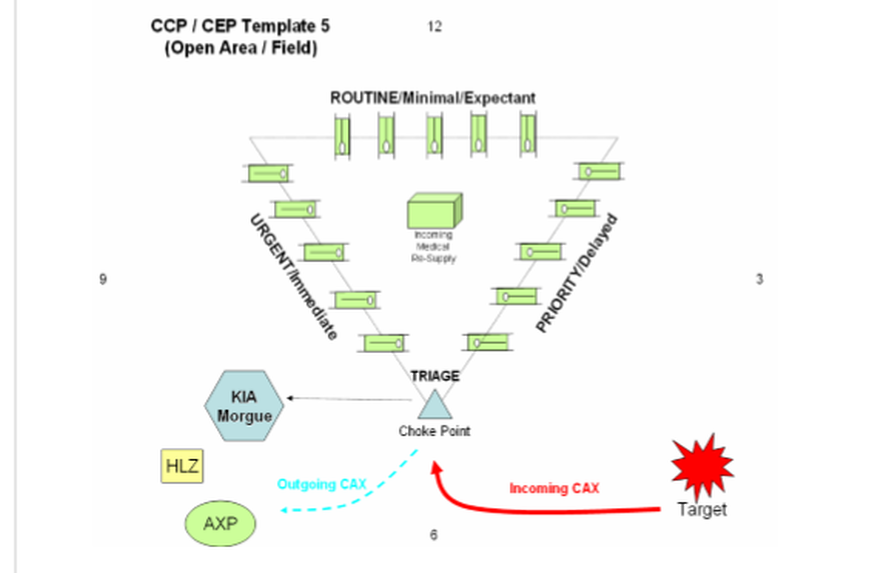
Traditionally, CCPs take a triangular form like so, especially in the field or open area:
Other shapes include:
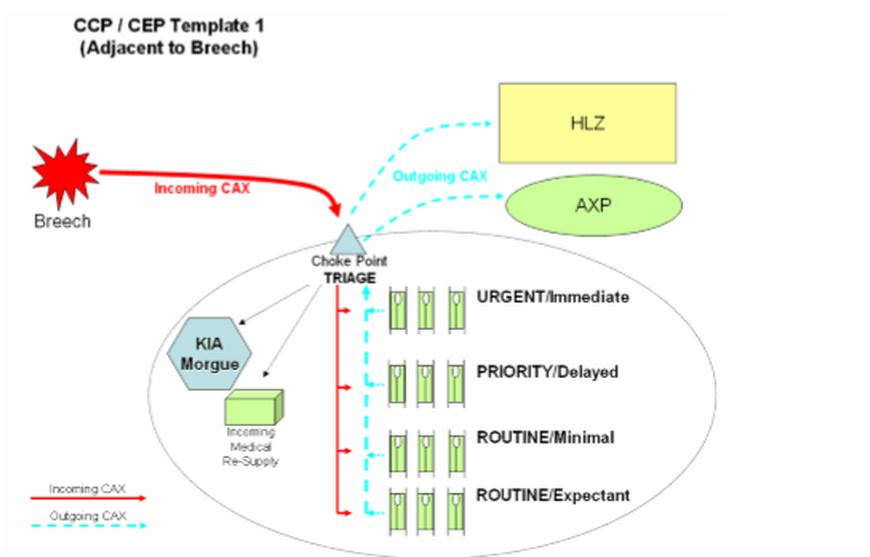
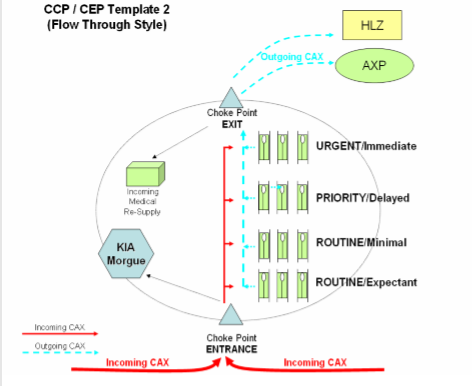
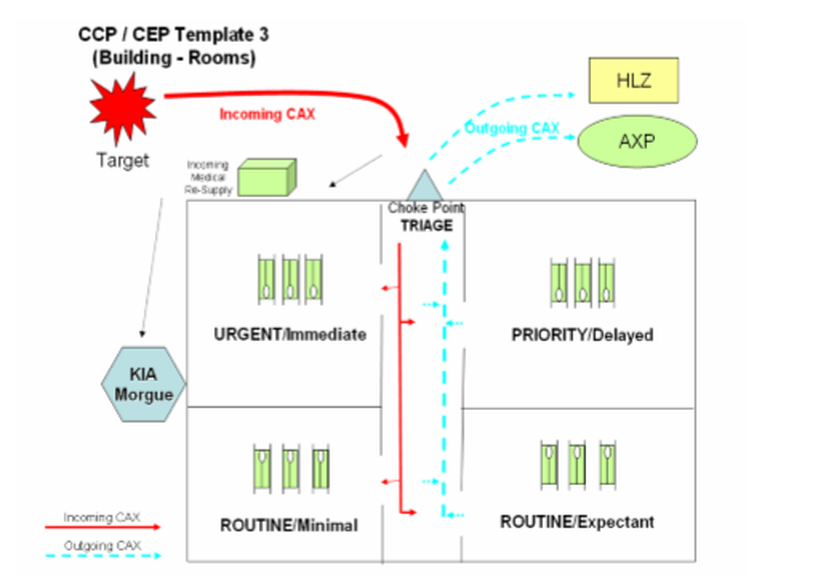
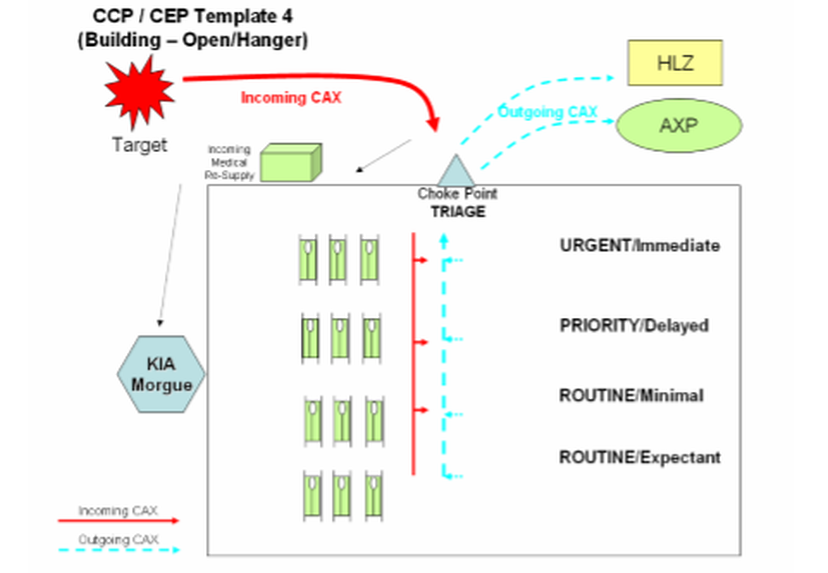
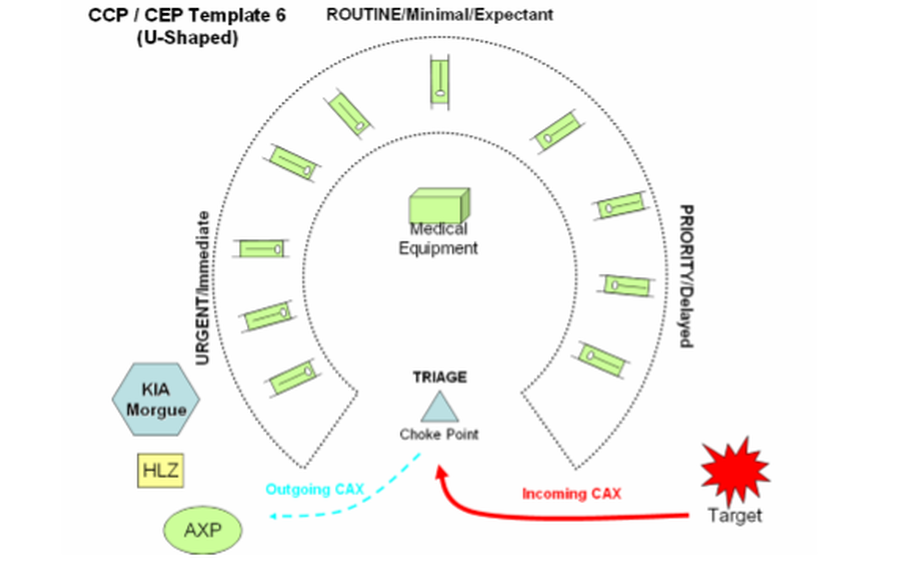
Many times, the CCP location/shape/layout is dictated by the conditions on the ground
It is important to remain flexible to achieve mission completion.
It is important to remain flexible to achieve mission completion.
Locations

CCPs can be located almost anywhere, however the overall security of the patients is paramount in site selection
By nature, a CCP is highly vulnerable to enemy action and so site location coupled with noise and light discipline is paramount while operating in contested territory
The most common site locations are:
• In a concealed field location
• In an abandoned house (UO - Urban Operations)
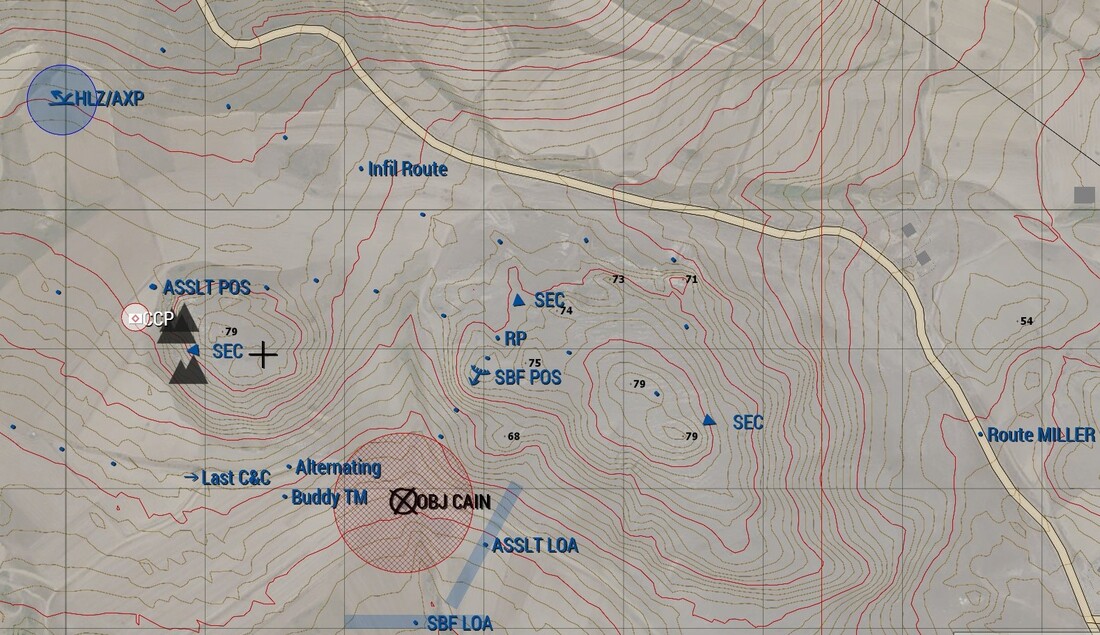
It is important to place the CCP along the natural 'drift of travel' of the fighting force. This will make it easier for patients to move to the CCP in case of need.
During classic operations such as a raid, the CCP can be placed at an ORP or closer to assault positions, as they are more likely to sustain the majority of casualties.
By nature, a CCP is highly vulnerable to enemy action and so site location coupled with noise and light discipline is paramount while operating in contested territory
The most common site locations are:
• In a concealed field location
• In an abandoned house (UO - Urban Operations)
It is important to place the CCP along the natural 'drift of travel' of the fighting force. This will make it easier for patients to move to the CCP in case of need.
During classic operations such as a raid, the CCP can be placed at an ORP or closer to assault positions, as they are more likely to sustain the majority of casualties.
Main Components

All CCPs should have:
• 'Choke' point
• Triage area
• 3 levels of care (urgent/priority/routine)
• An evacuation point (HLZ/ground transport pick-up point)
• An area out-of-sight for KIA
• An area for 'walking wounded'
• An area for medical supplies/resupply
• 'Choke' point
• Triage area
• 3 levels of care (urgent/priority/routine)
• An evacuation point (HLZ/ground transport pick-up point)
• An area out-of-sight for KIA
• An area for 'walking wounded'
• An area for medical supplies/resupply

Critical Factors
These factors are critical to mission completion
***Security...Security...Security***
In Murphy's Law, it is stated that professional soldiers are predictable but the world is full of amateurs
That is to say that CCPs should not be targeted by enemy forces, but amateurs almost never follow the script.
***Security...Security...Security***
In Murphy's Law, it is stated that professional soldiers are predictable but the world is full of amateurs
That is to say that CCPs should not be targeted by enemy forces, but amateurs almost never follow the script.
Establish and maintain C2 (Command & Control)
• PLT CCP - PSG (Platoon Sergeant)
• CP CCP - 1SG (First Sergeant)
• PLT/CP Medic - Performs life saving treatments
• RTO - Maintains radio communication with higher HQ/MEDEVAC
• TCCC qualified personnel - Triage incoming casualties
• CP CCP - 1SG (First Sergeant)
• PLT/CP Medic - Performs life saving treatments
• RTO - Maintains radio communication with higher HQ/MEDEVAC
• TCCC qualified personnel - Triage incoming casualties
Sustain life saving treatments
This is normally performed by the PLT/CP Medic and or TCCC qualified personnel
Have 'positive control' over your supplies/equipment
Regardless of the rank of the individual patients, the CCP OIC/NCOIC are overall responsible. This includes medical supplies, patient equipment and KIA.
***Maintain positive control of casualties sensitive items (weapons; NVGs; GPS etc.)***
***Maintain positive control of casualties sensitive items (weapons; NVGs; GPS etc.)***
Maintain proper accountability
The CCP OIC/NCOIC MUST maintain a record of:
• NAME/RANK/UNIT
• Time received/time discharged/sent to MEDEVAC etc.
• A list of all injuries
• A list of all administered medicines
• A Battle Roster (BR) of all KIA
• An attached TC3 card/'Casualty Feeder' form
• NAME/RANK/UNIT
• Time received/time discharged/sent to MEDEVAC etc.
• A list of all injuries
• A list of all administered medicines
• A Battle Roster (BR) of all KIA
• An attached TC3 card/'Casualty Feeder' form
Communications
Whether it be radio or messenger or other form, positive communication with higher HQ/MEDEVAC must be present.
CCP Markings
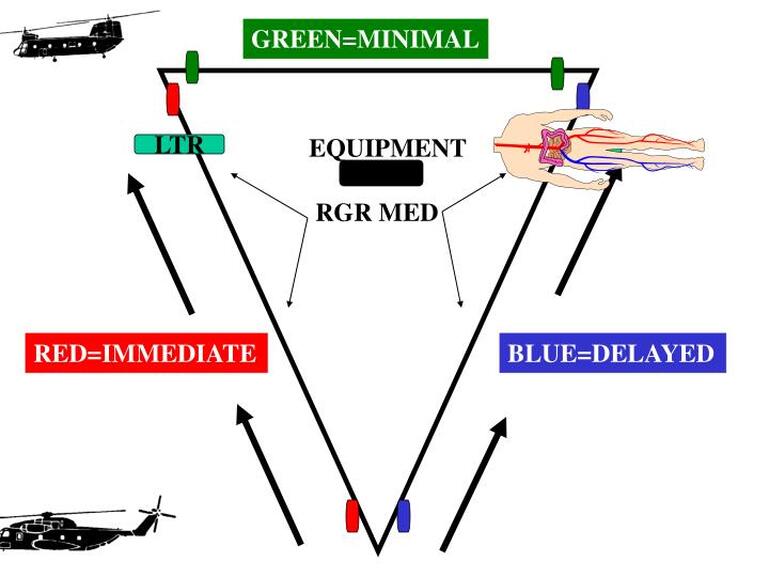
When in the traditional triangle shape the following colors apply:
• RED - Immediate/Critical (Urgent & Urgent-Surgical)
• BLUE - Delayed/Priority
• GREEN - Expectant/Routine
• None - Walking wounded/Routine
• RED - Immediate/Critical (Urgent & Urgent-Surgical)
• BLUE - Delayed/Priority
• GREEN - Expectant/Routine
• None - Walking wounded/Routine
Most times, 2 IR chemlights (tape/ties etc.) in the shape of a cross are used to signal the CCP location
If not, a yellow chemlight is used to mark the entrance or a cross is drawn using chalk
If not, a yellow chemlight is used to mark the entrance or a cross is drawn using chalk
Triage Categories and Color Markings

Basic categories are:
• URGENT/Immediate (to save life, limb or eyesight)
Red
• PRIORITY/Delayed (up to 4 hrs survival)
Yellow
• ROUTINE/Minimal (up to 24 hrs survival)
Blue
• ROUTINE/Expectant (moved as last group)
Green
***As unfortunate as it is to say but 'expectant' personnel should only be made as comfortable as possible. Excess time/energy/resources should not be given to them as this will lessen the survival chances of other personnel***
• URGENT/Immediate (to save life, limb or eyesight)
Red
• PRIORITY/Delayed (up to 4 hrs survival)
Yellow
• ROUTINE/Minimal (up to 24 hrs survival)
Blue
• ROUTINE/Expectant (moved as last group)
Green
***As unfortunate as it is to say but 'expectant' personnel should only be made as comfortable as possible. Excess time/energy/resources should not be given to them as this will lessen the survival chances of other personnel***
Forms
There are 2 main CCP forms for field use:
• TC3 - Tactical Combat Casualty Care card
• Casualty Feeder form
EVERY servicemember must use their TC3 cards on them in their First Aid pouch
When a servicemember is injured you must use their card...not yours
TC3 forms have an attached rubber band to secure to the servicemember
Have a wax pencil that is semi-permanent to write on the card(s)
Have a permanent marker to write on wounded personnel (T=tourniquet; M=morphine etc.)
Casualty Feeder forms are filled out by Medics/Leaders
• TC3 - Tactical Combat Casualty Care card
• Casualty Feeder form
EVERY servicemember must use their TC3 cards on them in their First Aid pouch
When a servicemember is injured you must use their card...not yours
TC3 forms have an attached rubber band to secure to the servicemember
Have a wax pencil that is semi-permanent to write on the card(s)
Have a permanent marker to write on wounded personnel (T=tourniquet; M=morphine etc.)
Casualty Feeder forms are filled out by Medics/Leaders
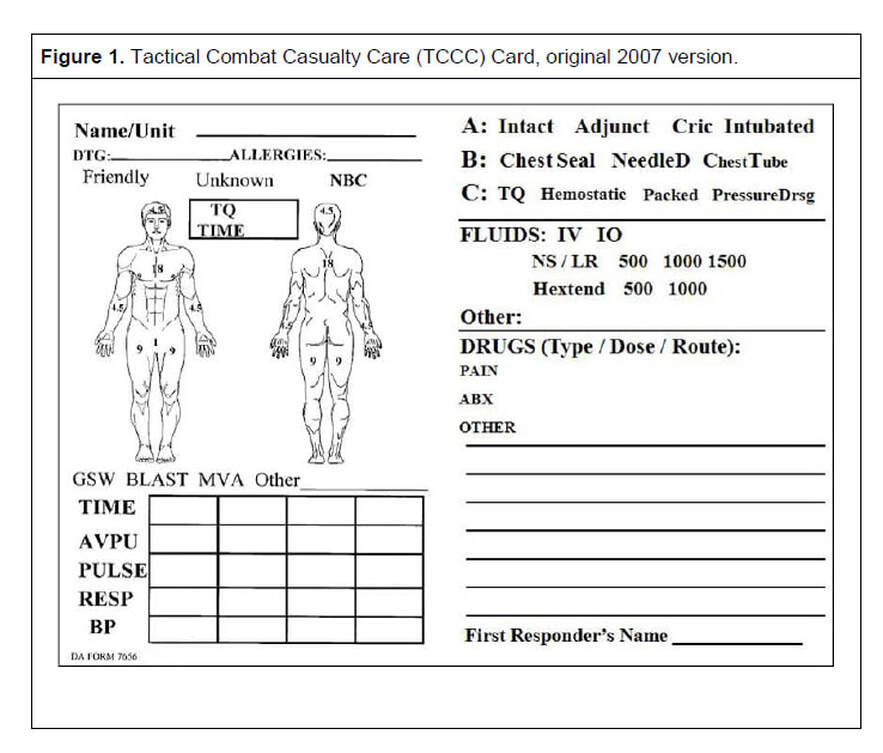
TC3 Card - Lists the patient's:
• Name/rank/unit
• Administered drugs
• Treatment given
• Mechanism Of Injury (MOI) such as gun shot wound, burn percentage, etc
• Vital signs
***TC3 Cards MUST remain attached to the patients***
• Name/rank/unit
• Administered drugs
• Treatment given
• Mechanism Of Injury (MOI) such as gun shot wound, burn percentage, etc
• Vital signs
***TC3 Cards MUST remain attached to the patients***
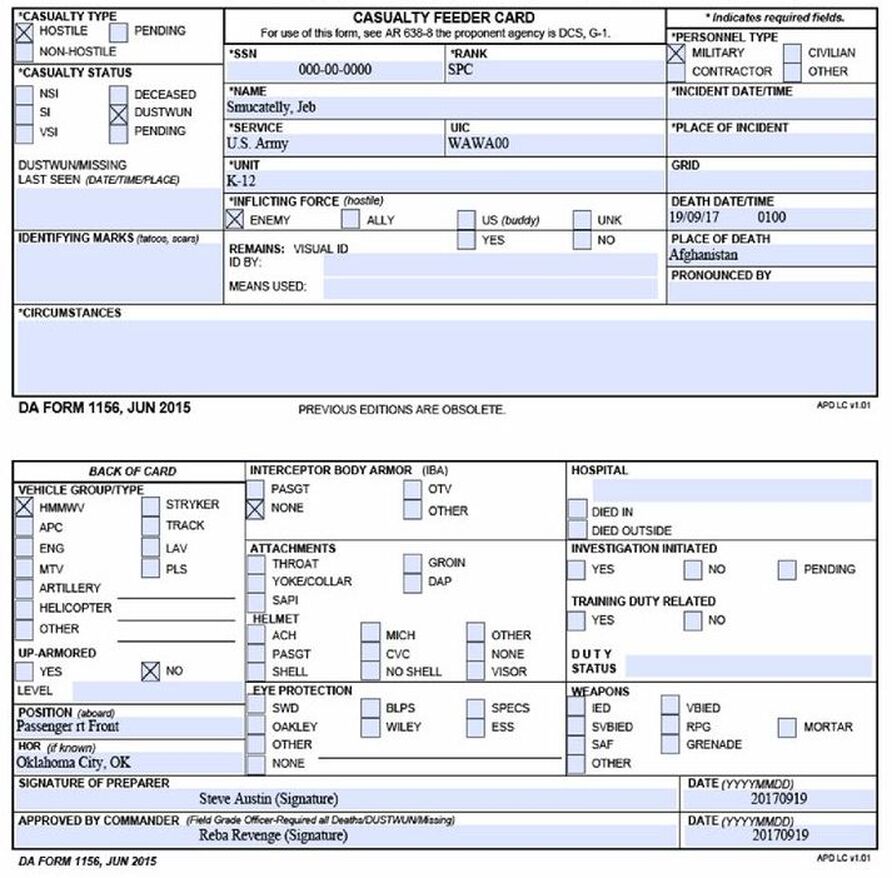
This card is used to inform higher HQ as to a servicemember's status
Common examples include:
• Deceased (KIA)
• NSI/SI/VSI (Not Seriously Injured/Seriously Injured/Very Seriously Injured)
• DUSTWUN (Duty Status Whereabouts Unknown) for MIAs
Common examples include:
• Deceased (KIA)
• NSI/SI/VSI (Not Seriously Injured/Seriously Injured/Very Seriously Injured)
• DUSTWUN (Duty Status Whereabouts Unknown) for MIAs
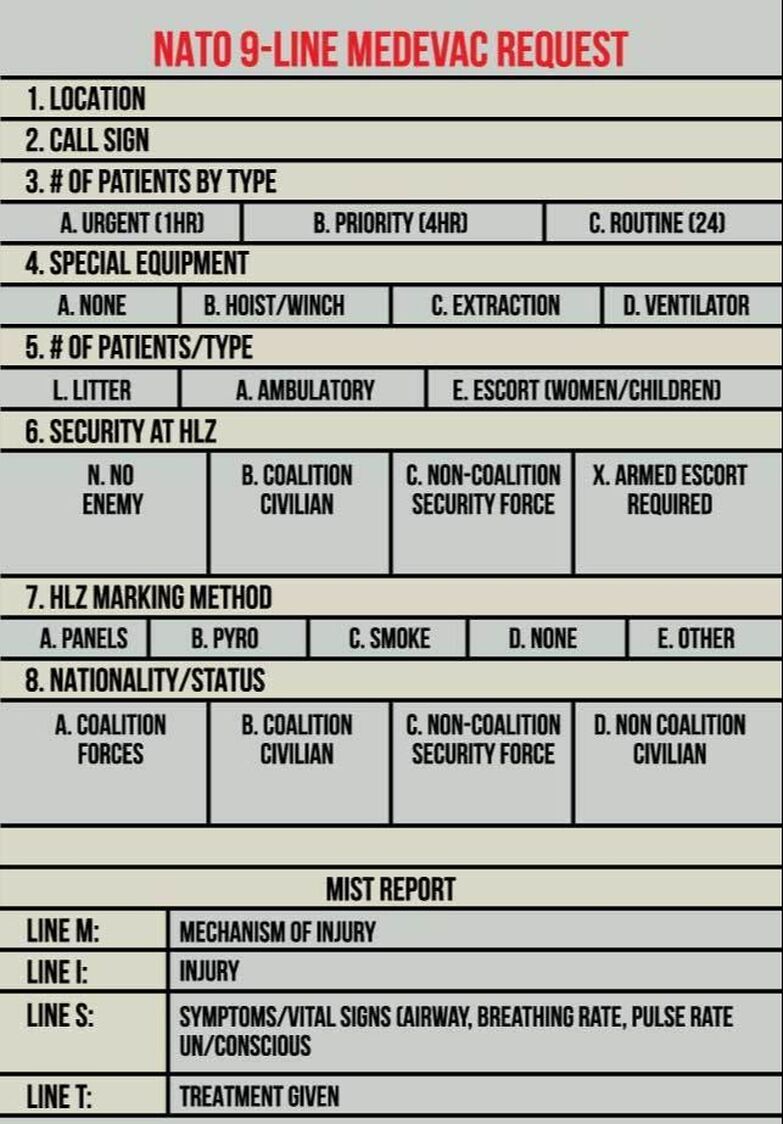
9-Line MEDEVAC
CCP Tactics, Techniques & Procedures
KIAs
• If possible, separate KIA from visual sight of other WIA. This can be achieved by placing them in a separate room or by using a poncho(s) to mask their sight
• KIAs should be place in a 'body bag'; covered by a poncho(s) or at the very least be hidden from sight
Urgent/priority placement
• The 'Urgent/priority' part of the CCP should be closest to the HLZ/AXP
• Use chemlights/chalk powder/colored cloth etc. to mark CCP categories (urgent/routine/minimal)
Unit training
- Practice CCP site selection/creation/manning/breakdown as a unit
• If possible, separate KIA from visual sight of other WIA. This can be achieved by placing them in a separate room or by using a poncho(s) to mask their sight
• KIAs should be place in a 'body bag'; covered by a poncho(s) or at the very least be hidden from sight
Urgent/priority placement
• The 'Urgent/priority' part of the CCP should be closest to the HLZ/AXP
• Use chemlights/chalk powder/colored cloth etc. to mark CCP categories (urgent/routine/minimal)
Unit training
- Practice CCP site selection/creation/manning/breakdown as a unit
CCP Manning
CCP are generally manned in the following manner:
• The PSG/1SG is the overall responsible for the CCP. They manage site location; local security; personnel/equipment/sensitive items accountability; HLZ/AXP set-up; communications with higher HQ
• Choke point/Triage is manned by a TC3 qualified trooper that identifies the level of care needed
• The PLT/COY medic/senior medic treats the casualties in order of urgency (immediate/priority/routine/expectant)
• Other TC3 qualified personnel assist in Buddy Aid
• RTO handles communications with higher HQ and 'Dust-Off' (MEDEVAC)
• 2 or more personel to clear an HLZ/AXP for MEDEVAC; act as ground guide and transport WIA/KIA
• Fireteam / Squad(s) to provide local security
• A servicemember to collect sensitive items/weapons/ammunition/equipment of WIA/KIA
• The PSG/1SG is the overall responsible for the CCP. They manage site location; local security; personnel/equipment/sensitive items accountability; HLZ/AXP set-up; communications with higher HQ
• Choke point/Triage is manned by a TC3 qualified trooper that identifies the level of care needed
• The PLT/COY medic/senior medic treats the casualties in order of urgency (immediate/priority/routine/expectant)
• Other TC3 qualified personnel assist in Buddy Aid
• RTO handles communications with higher HQ and 'Dust-Off' (MEDEVAC)
• 2 or more personel to clear an HLZ/AXP for MEDEVAC; act as ground guide and transport WIA/KIA
• Fireteam / Squad(s) to provide local security
• A servicemember to collect sensitive items/weapons/ammunition/equipment of WIA/KIA

For units smaller than a platoon/company, the same principles apply but the scale of the CCP is sized down
For units larger than a platoon/company, the same principles apply but the scale of the CCP is enlarged
For units larger than a platoon/company, the same principles apply but the scale of the CCP is enlarged
Task Organization

Scenario Example
Platoon conducting a deliberate raid
• 3 Rifle Squads
• 1 Weapon Squad
• 1 HQ element (OIC/NCOIC/RTO/Medic)
• 1 Weapon Squad
• 1 HQ element (OIC/NCOIC/RTO/Medic)
Initial assault:
• Assault section - 1st Squad plus OIC
• Support by Fire - Weapon Squad plus NCOIC plus RTO
• Security - 2nd Squad
• Reserve - Alpha Team/3rd Squad
• Medical/resupply - Bravo TM/3rd Squad plus medic
• Assault section - 1st Squad plus OIC
• Support by Fire - Weapon Squad plus NCOIC plus RTO
• Security - 2nd Squad
• Reserve - Alpha Team/3rd Squad
• Medical/resupply - Bravo TM/3rd Squad plus medic
Actions On the Objective (AOO):
• Assault reaches its limit of advance
• Support by Fire relocates to its limit of advance
• Security blocks off the objective
• Reserve - transports injured to CCP and takes their place in combat
• Medical/resupply - treats the injured at the CCP and resupplies as needed
• Assault reaches its limit of advance
• Support by Fire relocates to its limit of advance
• Security blocks off the objective
• Reserve - transports injured to CCP and takes their place in combat
• Medical/resupply - treats the injured at the CCP and resupplies as needed
The objective is secured and the unit exfiltrates:
• Injured unit members meet at the CCP
• MEDEVAC is requested
• An HLZ/AXP is set up at the predetermined point
• The unit CMs/RTB etc.
• The unit moves/meets at the ORP
• Reorganize/reconsolidate
• CMs/RTB etc.
• Injured unit members meet at the CCP
• MEDEVAC is requested
• An HLZ/AXP is set up at the predetermined point
• The unit CMs/RTB etc.
• The unit moves/meets at the ORP
• Reorganize/reconsolidate
• CMs/RTB etc.
• PSG - HLZ/AXP kit and CCP markings (chemlights/panels etc.)
• Medic - Aid bag
• TC3 - Squad aid bag/casualty equipment bag
• RTO - Radio/9-line MEDEVAC
• Trooper - first aid pouch
• Medic - Aid bag
• TC3 - Squad aid bag/casualty equipment bag
• RTO - Radio/9-line MEDEVAC
• Trooper - first aid pouch
***Actions to take before an operation:***
• Sufficient stretcher fabrication
• HLZ/AXP site selection/preparation
• CCP site selection/preparation
• Medical supply consolidation
• HLZ/AXP site selection/preparation
• CCP site selection/preparation
• Medical supply consolidation

CCP Related Equipment
Fabricate sufficient stretchers with just a standard poncho/BDUs or other basic materials
Folded tactical stretcher

SKEDCO portable litter

2x BDU with wooden poles

Tactical 'soft' stretcher - 1 per squad


Body Bag - 1 per squad

Casualty Equipment Bag - 1 per squad

|

|
Medic Kit Bag - Medic only
(advanced medical training)
(advanced medical training)

First Aid bag - TC3 qualified combat life saver

Individual First Aid Kit - Every member

Medical Training
"The combat medic specialist is primarily responsible for providing emergency medical treatment at point of wounding on the battlefield, limited primary care, and health protection and evacuation from a point of injury or illness"
Job duties:
• Administer emergency medical treatment to battlefield casualties
• Assist with outpatient and inpatient care and treatment
• Instruct personnel on the Combat Lifesaver/First Responder training course
• Manage medical readiness, medical supplies and equipment
Training:
6 months of specialized training including:
• Patient-care techniques
• Emergency medical techniques
• Advanced medical care
• Plaster-casting techniques
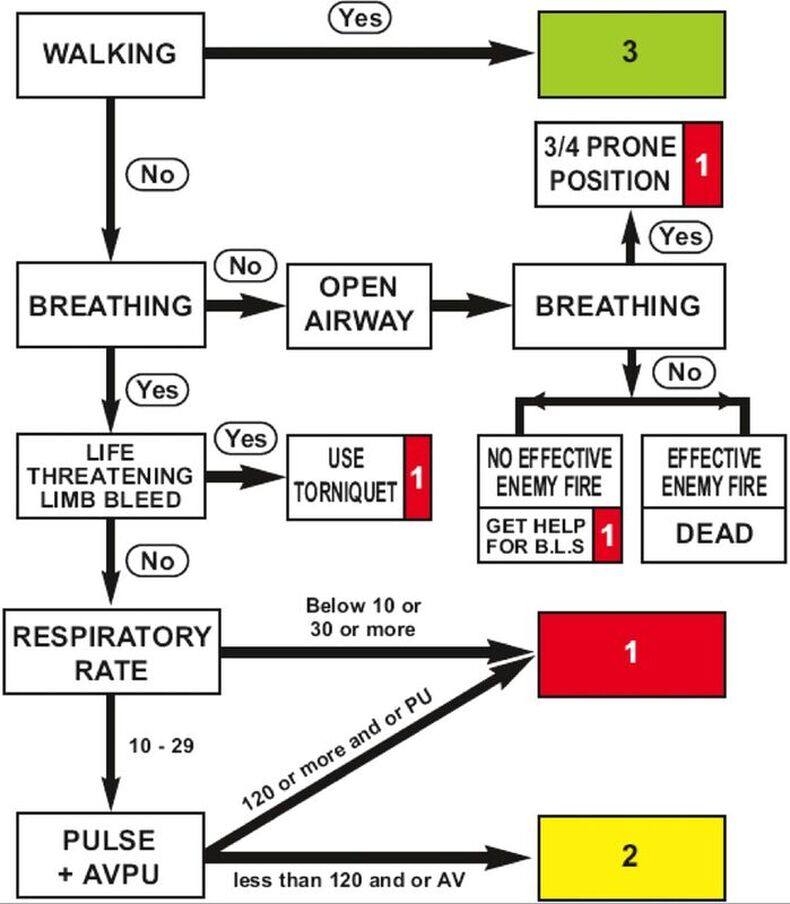
Tactical Combat Casualty Care
"TCCC teaches first responders to treat casualties in the proper order,treating the most critical situations first. This is done using the acronyms MARCH and PAWS"
MARCH
"Massive hemorrhage, Airway, Respirations, Circulation, Head injury/Hypothermia is an acronym used by TCCC-trained individuals to help remember the proper order of treatment"
PAWS
"Pain, Antibiotics, Wounds, Splinting is an acronym used by TCCC trained individuals to help remember additional casualty care issues"
Job duties:
• Administer emergency medical treatment to battlefield casualties
• Assist with outpatient and inpatient care and treatment
• Instruct personnel on the Combat Lifesaver/First Responder training course
• Manage medical readiness, medical supplies and equipment
Training:
6 months of specialized training including:
• Patient-care techniques
• Emergency medical techniques
• Advanced medical care
• Plaster-casting techniques
Tactical Combat Casualty Care
"TCCC teaches first responders to treat casualties in the proper order,treating the most critical situations first. This is done using the acronyms MARCH and PAWS"
MARCH
"Massive hemorrhage, Airway, Respirations, Circulation, Head injury/Hypothermia is an acronym used by TCCC-trained individuals to help remember the proper order of treatment"
PAWS
"Pain, Antibiotics, Wounds, Splinting is an acronym used by TCCC trained individuals to help remember additional casualty care issues"
Conclusion
The use of a CCP greatly increases the survivability rate of personnel on the battlefield
Make sure to rehearse the creation/use/break down of a CCP
Platoon and Company sized elements are best to deploy a CCP
Know ahead of time what each member is responsible for (triage/MEDEVAC/litter/etc.)
Make sure to rehearse the creation/use/break down of a CCP
Platoon and Company sized elements are best to deploy a CCP
Know ahead of time what each member is responsible for (triage/MEDEVAC/litter/etc.)